Playlist
Show Playlist
Hide Playlist
Tuberculous Meningitis


-
Slides 10 CNSInfections Neuropathology I.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
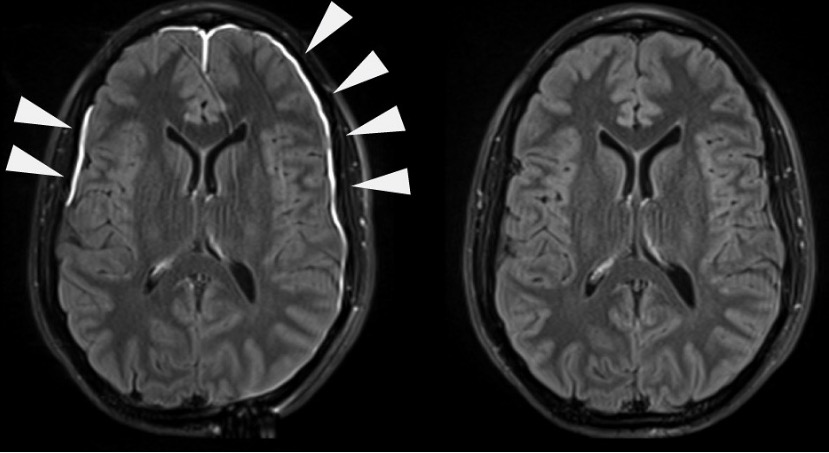
00:01 We’re moving on to tuberculous meningitis. 00:03 So tuberculosis. 00:05 And so when you say tuberculosis meningitis, keep in mind that granted, it is bacterial. 00:09 However -- However, I need you to keep this separate from the other bacterial causes that I’d walk you through based on the age groups Are you with me? Remember that table that I gave you where it was predisposing factors, but it was age groups, right? And I gave you specifically those bacteria. 00:27 You’ll notice that in that second column, that there is no tuberculosis there because you’re keeping it separate. 00:34 If you do that for me clinically, you’ll be in good shape. 00:37 Now, the onset here will be insidious. 00:40 Your typical symptoms that you would expect, photophobia, headaches, so on and so forth. 00:44 And here, it causes a? Please focus on basilar meningitis. 00:51 In other words, secondary angiitis could also be possible because of its location. 00:58 Is that clear? The most important point in this slide, in this section, is going to be that last statement of where it’s affecting your meninges. 01:09 And what you’re finding here on your CT, now granted, in your particular point in education that by looking at the CT, you would need to have proper history so that you would then identify what you find in that arrow as being the actual pathology. 01:27 Let’s continue. 01:28 Complications: They may result in hydrocephalus, but for the most part, whenever you have meningitis, at some point in time, you’re going to scar. 01:39 You could scar the arachnoid granulation. 01:42 Picture that for me. 01:43 Close your eyes. 01:44 Are you with me? Arachnoid granulation, where are you? Subarachnoid space and this will be the drainage point of your cerebrospinal fluid. 01:53 What if you scar them? If you scar them and if you’re not familiar with the concept of hydrocephalus, this will a communicating, nonobstructive type of hydrocephalus. 02:04 What did I say? Communicating. 02:06 Why? Don’t worry. It’s to come. 02:11 And it’s nonobstructive. 02:12 Why? Also an explanation that I’ll give to you when the time is right. 02:18 Stroke: what happened here? Remember, you could have blood vessels that are affected, interesting. 02:26 And with stroke, what does that mean to you? It means that there is a lack of blood supply to whatever part of the brain. 02:33 So if you know for a fact that tuberculosis or tuberculous meningitis could affect the basilar part of your brain, and you could then affect adjacent and result in angiitis, specifically causing obliterative endarteritis. 02:46 What does that mean to you? It means inflammation of the innermost layer of the arteries, which can lead to occlusion and decreased blood flow to the tissue or organ that the artery supplies. 02:56 Here, we're gonna evaluate the supraspinal fluid for tuberculosis or tuberculous meningitis. 03:02 Keep this separate from all the others because the findings here are going to be a little bit different. 03:07 Here, predominantly, your WBCs will be lymphocytes. 03:10 Where else would you find lymphocytes, perhaps? Viruses. Interesting. So, you find tuberculosis being a mix between bacterial and viruses. 03:20 Do that for me? You'll be in good shape. In bacterial, what kind of WBC would you expect to find? Good, neutrophil. RBCs, none. When did we see RBCs in supraspinal fluid? Oh, yeah, encephalitis or maybe brain abscess, meaning to say, parenchyma involvement. 03:42 Look at this, glucose. Concept. This is microbacteria. 03:48 There you go. So, what is it going to do with glucose? Consume it. Interesting. 03:54 So, I told you, with tuberculous meningitis, it's a hybrid in terms of CFS findings between your viruses, lymphocytes, bacterial with neutrophils. 04:05 Here in tuberculous, you find lymphocytes. 04:09 Bacterial, glucose, expect that to be decreased, as you see here. 04:13 In viruses, glucose will be relatively normal. 04:17 Protein, on the higher side, and that's pretty much you're seeing with any type of meningitis, but particularly higher with bacterial, and here we have tuberculous. Are we clear? So, in order for you to understand this slide, I would recommend that you understand your findings for bacterial viral -- viral meningitis first, then take a look at your CSF findings for tuberculous. let's continue. 04:44 Let's take a look at management of tuberculous meningitis. 04:47 This obviously keeps advancing but at this point, at least know the basics. 04:51 Ripe, R-I-P-E, and R referring to refampin, I, INH, P, pyrazinamide, E, ethambutol, and of course, you know about INH in all its glory in terms of causing sideroblastic anemia. All right? Maybe consider moxiflox or moxifloxacin, steroids, obviously if you're talking about taking care of the inflammation, and you wanna think about giving more or less, a drainage, alright, so you have your ventriculostomy for hydrocephalus. 05:23 Always a possibility, isn't it? Surgical decompression if required, for sure, because of that increased intracranial pressure. 05:31 Management of tuberculous meningitis in greater detail, know it well. Know it well.
About the Lecture
The lecture Tuberculous Meningitis by Carlo Raj, MD is from the course CNS Infections - Clinical Neurology.
Included Quiz Questions
A 45-year-old man presents to the ER with a headache. He has a history of fever, night sweats, and weight loss for the last six months. A physical examination reveals photophobia and flexion of the hip and knees upon flexion of his neck. Which type of pathology is most likely seen in his condition?
- Basilar meningitis
- Aseptic meningitis
- Viral meningitis
- Parasitic meningitis
- Amebic meningitis
What is the drug of choice in the treatment of severe focal edema of the brain in a patient with tuberculous meningitis?
- Dexamethasone
- Surgical decompression
- Rifampicin
- Moxifloxacin
- Ventriculostomy
Which of the following is not a complication of tuberculous meningitis?
- Obstructive hydrocephalus
- Non-obstructive hydrocephalus
- Stroke
- Obliterative endarteritis
- Scarring of arachnoid granulations
What is the pathology behind stroke in a patient with tuberculous meningitis?
- Inflammation of the innermost layer of the arteries of the brain
- Inflammation of the outermost layer of the arteries of the brain
- Inflammation of the innermost layer of the arteries of the spinal cord
- Inflammation of the outermost layer of the arteries of the spinal cord
- Inflammation of the middle layer of the arteries of the brain
Author of lecture Tuberculous Meningitis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Great stuff! Used lecturio before and after my exam. They have been constantly improving
