Playlist
Show Playlist
Hide Playlist
Subdural Hematoma: Diagnosis and Management

-
Slides Head Trauma Subdural Hemorrhage.pdf
-
Download Lecture Overview
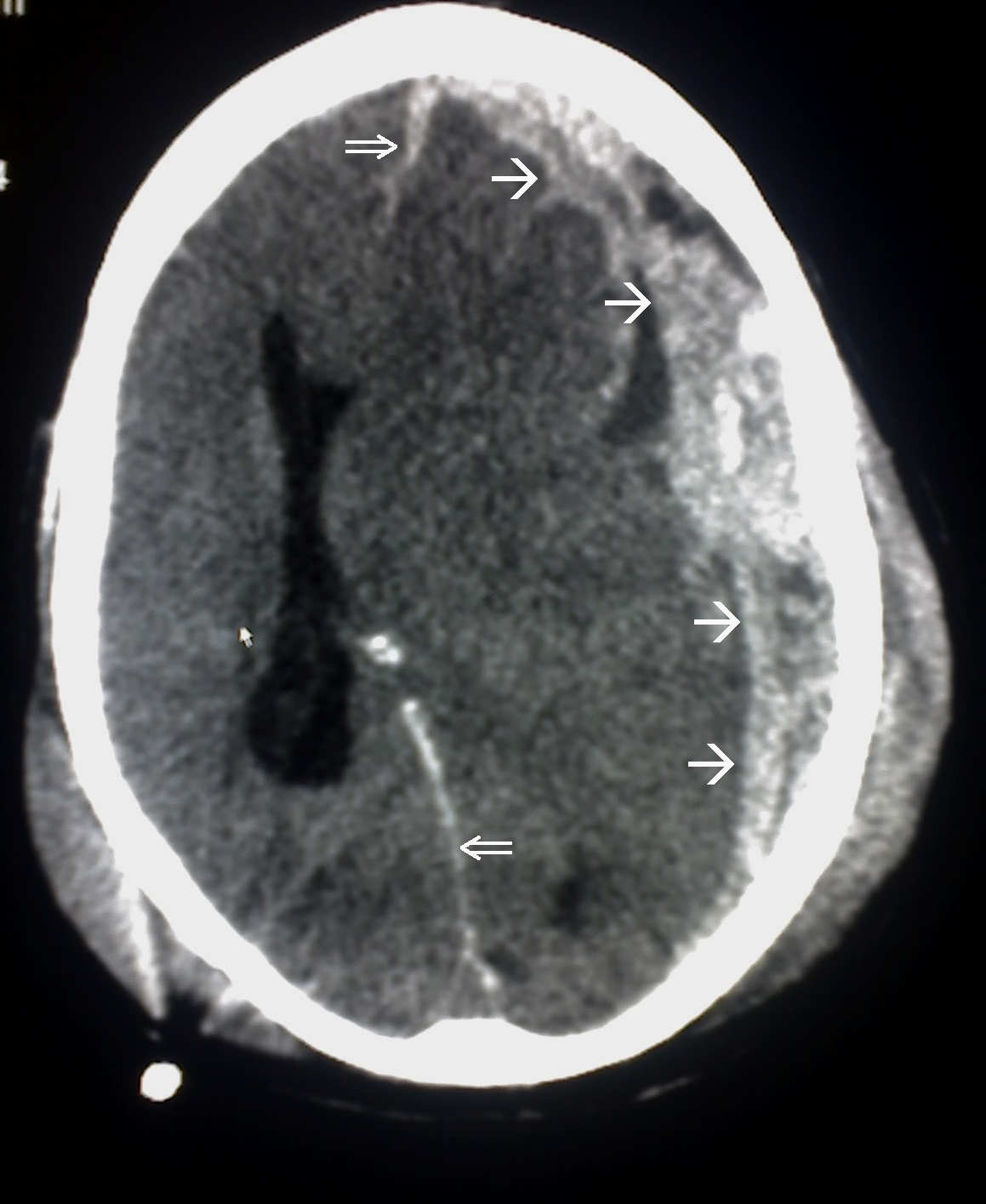
00:01 How about the diagnosis? How do we evaluate and diagnose these patients? Well as with all hemorrhages in the brain, the non-contrast head CT is the modality of choice. 00:10 In the acute setting, we see some significant hyper dense blood. 00:14 This appears as high density crescent-shaped collection of blood along the convexity and you can see that here in this non-contrast head CT over the surface of the left convexity. 00:24 Fresh blood appears as a high density on CT. 00:30 Subacute and chronic subdurals appear more iso or hypodense, still a crescent collection of blood over the surface of the brain. 00:39 But here are the blood is iso or hypodense. 00:42 Blood collections in this stage are often more difficult to distinguish from the surrounding anatomy and can be seen but particularly small subdural collections require a careful eye and an interrogation of the CT. 00:58 We can see subdural develop anywhere in the brain unilateral subdurals create distortion of the cerebral contour and affect the brain underlying the subdural. 01:08 In the setting of bilateral subdural, this may create significant increases in ICP, and that distortion of the brain may be a little bit less evident. 01:18 Here we see significant midline shift and it's obvious that we're dealing with a left sided subdural, but too small subdural may be difficult to appreciate the degree of increase in mass effect on the brain. 01:31 How about management? How do we manage these patients? Well, we use the same 6 steps for managing subdural as epidurals. 01:38 1. ACLS protocols manage airway breathing and circulation in patients who are presenting with significant symptoms. 01:46 This can result in life threatening injuries, both from the hematoma as well as the trauma that contributed to it and those should be addressed. 01:53 Immediate discontinuation of antiplatelets and anticoagulants is important. 01:57 We want to prevent the hematoma from expanding and these medicines could contribute to expansion and should be stopped or reversed. 02:05 Fourth, we want to undergo efforts to achieve and maintain hemodynamic stability. 02:10 Fifth, non-contrast head CT should be performed as soon as possible. 02:14 And sixth, emergent neurosurgical consultation is needed particularly in patients with low GCS or significant focal neurologic deficits or a concern for increased ICP. 02:25 How about non-operative management? What do we think about from non-operative management of subdurals? Well, this may be appropriate for patients with more favorable Glasgow Coma scales who are clinically stable. 02:36 With small subdural is less than 10 mm in greatest thickness on the head CT or the absence of brain herniation signs are significant focal neurologic deficits. 02:47 Even a small deficit may be a reason for surgical intervention. 02:50 Asymptomatic patients can undergo non-operative management. 02:56 Patients should be monitored in a neurological ICU, particularly if they're more severe symptoms or patients who are on anticoagulation and the hematoma typically resolves within several weeks. 03:05 4-6 weeks, it may take or even longer for reabsorption of the blood. 03:11 Operative management may be appropriate in selected patients, particularly those with low GCS who are considered unstable with large hematoma is more than 10 mm in their maximum thickness on the CT. 03:24 In patients who are higher risk for brain herniation or with increased intracranial pressure. 03:31 The types of operative management that we would consider include surgical techniques like craniotomy for hematoma evacuation, a burr hole to evacuate blood in a less invasive procedure, a decompressive craniectomy, particularly if there's underlying trauma to the brain and cerebral edema, or subdural evacuation through a port system. 03:50 Culprit vessels can be identified and tamponade at the time of surgery. 03:55 However, in the vast majority of patients, the blood will tamponade and stop bleeding on its own.
About the Lecture
The lecture Subdural Hematoma: Diagnosis and Management by Roy Strowd, MD is from the course Head Trauma.
Included Quiz Questions
What imaging findings are seen on a non-contrast head CT in a patient with subdural hematoma?
- High-density crescent-shaped collection at the convexity
- High-density lens-shaped collection at the convexity
- Paraventricular hockey stick lesions
- High-density crescent-shaped collection in the ventricles
- High-density lens-shaped collection in the ventricles
After stabilization using ACLS protocol and addressing life-threatening injuries, what is the next step in managing a patient with a subdural hematoma?
- Discontinuing and reversing anticoagulants
- Repeating imaging
- Neurosurgical consultation
- Hyperventilation
- Placement of an ICP monitor
A patient presents with subdural hematoma, and the emergency department physician consults neurosurgery based on the size of the hematoma. What is the threshold for consideration of operative management in a patient with a subdural hematoma?
- 10 mm
- 8 mm
- 12 mm
- 6 mm
- 5 mm
Author of lecture Subdural Hematoma: Diagnosis and Management

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
