Playlist
Show Playlist
Hide Playlist
Secondary Skin Lesions

-
Slides Secondary Skin Lesions.pdf
-
Download Lecture Overview
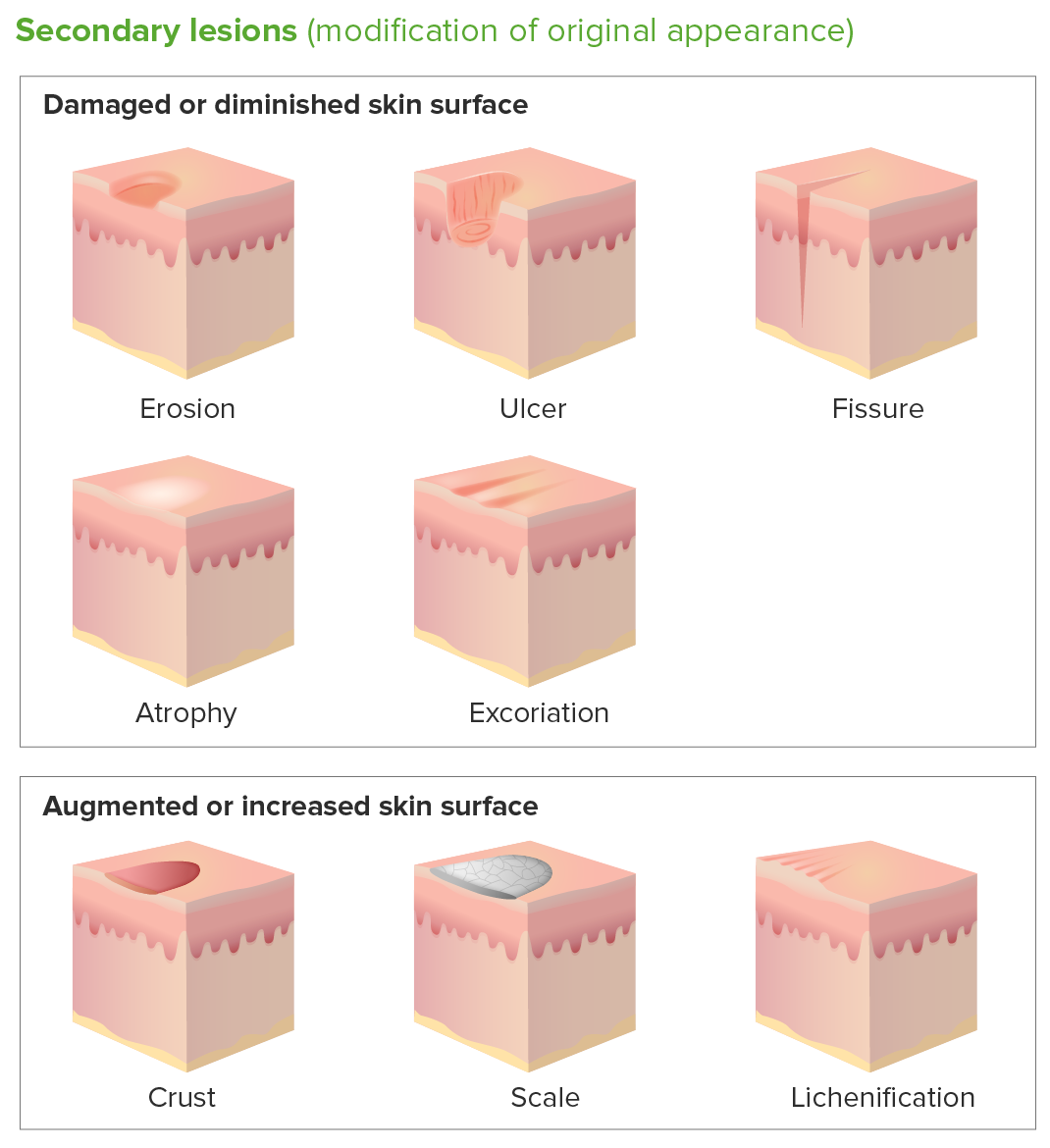
00:01 So we want to talk now about secondary lesions. 00:03 We've finished discussing primary lesions. 00:06 We're moving on to secondary lesions a crust it is a dried serum can be serous blood or pus on the surface of the skin. 00:17 It may include bacteria typically Staphylococcus aureus which we find on the skin. Here are some examples of crusts. 00:26 This is a patient with impetigo secondarily infected with staph aureus bacteria, resulting in crusting which we have just described. 00:36 The color may be honey colored or it may be hemorrhagic. 00:41 The next topic is about the next type is scale. 00:46 In a scale, what do we see? We see hyperkeratosis that is thickening of the skin, and this is due to accumulation of stratum corneum due to increased proliferation and or delayed desquamation. 00:59 These are some examples of scale. 01:02 This is a patient with typical psoriasis vulgaris with silvery scales on the buttock area. Another type of scale is a patient with tinea corporis. 01:14 You can see an active annular scale on this picture. 01:20 A fissure. 01:21 This is a linear cleft in skin, and it's usually painful. 01:26 It results from marked drying, skin thickening, and loss of elasticity. 01:31 An example of a fissure is angular colitis. 01:35 We see angular colitis in patients who have either diabetes or immunocompromised from HIV. And sometimes it can be used to it can be used to ill feature fitting dentures. 01:50 Excoriation is an exogenous injury to all or part of the dermis. 01:55 It is usually due to scratching. 01:57 An example of an excoriation. 01:59 This is a young girl who's been picking the skin, resulting in excoriations. 02:05 You can also see excoriations in patients with atopic eczema who have intense pruritis, and they tend to pick and scratch on the skin. 02:14 The next type of secondary lesion is lichenification, which is due to a we call it acanthosis, which simply means thickening of the epidermis and accentuation of natural skin lines. So these tend to be the skin lines tend to be more obvious, and this results from repeated scratching or rubbing. 02:35 This is an example of a patient with a thickening of the skin or lichenification, because it's due to lichen planus, lichen planus is itchy, and patients who have like lichenification, it's usually due to itchy conditions. 02:53 The example here is that of a lichenification due You to chronic atopic dermatitis. As I mentioned, you tend to see lichenification in patients who have got intense pruritis of each. 03:07 An erosion is partial or sometimes complete loss of the epidermis, and it's moist, oozing and or crusted lesion. 03:16 This is a young patient with a staphylococcal scalded skin syndrome SS, where you see typical erosions due to the lifting of the epidermis. 03:27 You can actually see typical erosions in patients with pemphigus vulgaris when the blister is actually opened. 03:35 Ulceration involves deeper defect compared to an erosion loss of the entire epidermis and the superficial dermis. 03:45 The examples of accelerated ulceration are scrofula, edema, which is a type of cutaneous tuberculosis, and this is due to infection with the TB bacteria. 03:56 Another example of an ulcer is diabetic foot ulcer. 04:01 Moving on now to a atrophy. 04:05 This can be epidermal dermal or a combination of these two. 04:10 If it's epidermal, it means there's thinning of the epidermis, leading to wrinkling and shiny appearance. 04:16 When it's dermal, you get loss of the dermis, particularly the collagen and elastin, leading to a depression on the skin. 04:25 An example of this is, for example, patients with senile atrophy, where the skin is so thin because of the loss of collagen and photoaging. 04:35 Another example is anetoderma, where you also see wrinkling of the skin, almost like tissue paper. 04:42 What about scars? We all complain about scars when you've got acne or after injury, so this is an important aspect of dermatology. 04:50 So what do we mean by scar. 04:52 It's increased thickness of the damage caused by enhanced production of collagen by the fibroblasts. And remember we mentioned that we tend to get more fibroblasts in black skin or melanin rich skin than in light skin. 05:05 So automatically we do anticipate that we will have more keloids and scars in black skin. So this is an example of a scar. 05:16 How do you differentiate between a scar and a keloid? Scar is limited to the original wound margin. 05:24 That's what we call a hypertrophic scar. 05:27 And it can be painful. 05:29 And the keloid is hypertrophic scar that extends beyond the original wound margin. 05:37 And that's how you differentiate between the two. 05:39 And by the way, you can also get spontaneous keloid where there is no history of any wound. But patients get spontaneous keloid. 05:48 And we see this a lot amongst patients of skin of color.
About the Lecture
The lecture Secondary Skin Lesions by Ncoza Dlova is from the course Introduction to Dermatology.
Included Quiz Questions
A patient presents with multiple crusted skin lesions on the face. A bacterial culture is performed. Which bacterium is most likely to be isolated?
- Staphylococcus
- Pseudomonas
- Escherichia coli
- Mycobacterium
- Clostridium
Which of the following leads to the formation of a scale?
- Accumulation of stratum corneum due to increased proliferation and/or delayed desquamation.
- Hyperactive sebaceous glands producing excess oil.
- Inflammation of the dermal layer leading to blister formation.
- Breakdown of collagen fibers in the epidermis.
- Overproduction of melanin causing pigmentation clusters.
What best describes lichenification?
- Thickening of the epidermis and accentuation of natural skin lines.
- A loss of pigmentation in patches of skin.
- Formation of fluid-filled blisters on the skin surface.
- Redness and swelling due to acute inflammation.
- Thinning of the skin leading to easy bruising.
Author of lecture Secondary Skin Lesions

Ncoza Dlova
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
