Playlist
Show Playlist
Hide Playlist
Renal Stenosis and Fibromuscular Dysplasia

-
Slides 05 VascularMedicine advanced.pdf
-
Reference List Vascular Medicine.pdf
-
Download Lecture Overview
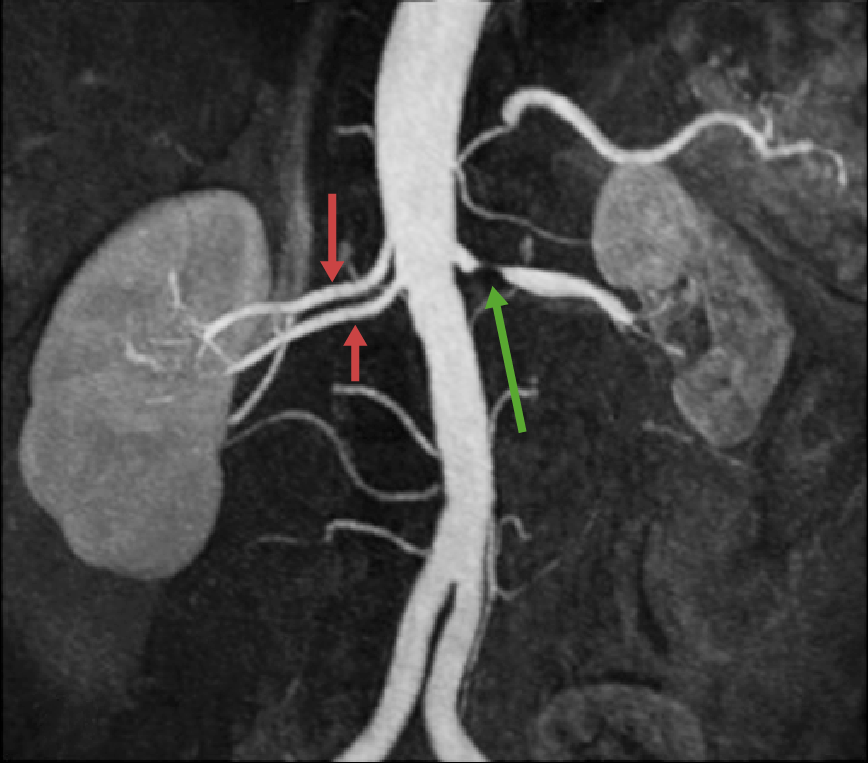
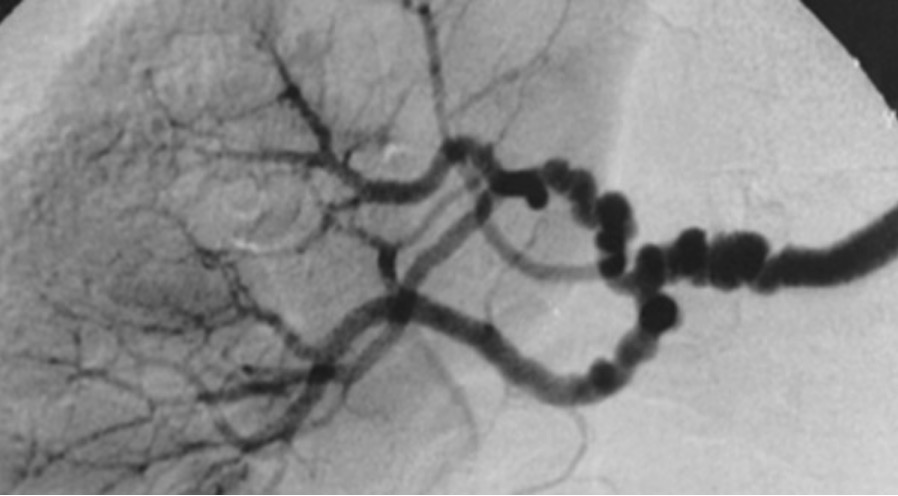
00:00 Let's talk, then, about a very common condition, renal stenosis, that can be caused either by atherosclerosis or a congenital condition known as fibromuscular dysplasia. And this is a discussion that's going to lead us into the next lecture, which is on hypertension. 00:19 Why? Because when we have disease in the kidneys, this frequently leads to high blood pressure and sometimes to difficult-to-control high blood pressure. 00:31 So let's talk, then, about renal artery stenosis. The definition is straightforward. It's a decrease in the diameter of the renal arteries. The lumen, or the channel, of the artery is narrowed. The commonest cause is atherosclerosis, as we've talked about with peripheral vascular disease. Of course, an embolus (a blood clot coming from the heart can… or from the aorta) can also lodge in the renal arteries and cause marked narrowing of the channel. But that's must less common compared to atherosclerosis, which is exceedingly common. There is a congenital form of renal artery stenosis known as arterial fibromuscular dysplasia. So what does that mean? "Fibromuscular" means fibrous, or scar, tissue and muscle. "Dysplasia" means abnormal development. So what happens here is that there's an abnormal development of fibrous tissue and smooth muscle tissue in the renal artery. That really only accounts for about 5% of renal artery stenosis; 95% are due to atherosclerosis. Again, we're going to say they're the risk factors for atherosclerosis. They're increased age. Now suddenly, you say, "Wait a minute: female? I thought males had atherosclerosis earlier." But when you're dealing with an increased aged population, remember, many of the men have died off, since men die before women. So when you look at a very elderly population anywhere—in Europe or the United States, anywhere in North America or South America—often, the elderly population is predominantly women, so that's why renal artery stenosis occurs… atherosclerotic renal artery stenosis occurs more common in women, because the women survive long enough to get it. 02:18 Hypertension is a very common cause, as you know, of atherosclerosis. Peripheral vascular disease—for example, intermittent claudication—tells you that there's atherosclerosis in the blood vessels… in the aorta and in the peripheral arteries, and very likely, there's going to be atherosclerosis in the renal artery. Patients with chronic kidney disease, where the blood tests show that kidney function is reduced: Often, one of the reasons for the reduced kidney function is renal artery atherosclerosis. Diabetes increases the risk for atherosclerosis, as you know, and also increases the risk for the development of renal artery atherosclerotic disease. Again, smoking: always a risk factor for increasing atherosclerosis. And, of course, again, abnormal lipid levels—high cholesterol levels—particularly high LDL cholesterol levels. All the things that predict increased atherosclerosis predict the likelihood that renal artery stenosis from an atherosclerotic cause may develop in an elderly patient. 03:25 The symptoms are often the symptoms of high blood pressure. Patients develop hypertension because of a mechanism known as the Goldblatt effect. Goldblatt was a renal physiologist in the early 20th century who did experiments on animals where he partially constricted the renal artery and showed that a substance was released from the kidney that caused high blood pressure. That substance is known as renin. We're going to have a lot of discussion of this in the next lecture on hypertension, because one of the common causes of hypertension is elevated renin. And again, the Goldblatt effect is because of a release of renin, because of a decreased diameter of the renal artery and, therefore, decreased blood supply into the kidney. And this leads to vasoconstriction and hypertension in the body—that is, the small arterioles clamp down, and there's hypertension. If a patient develops sudden deterioration in kidney function, this can often be because an atherosclerotic plaque has ruptured in the renal artery and a clot has formed, markedly decreasing the blood flow into the kidney—just like one can have a ruptured plaque in the coronary artery, leading to a myocardial infarction secondary to thrombosis. So again, just to take a few minutes to talk about fibromuscular dysplasia: That causes 5% of renal artery stenosis. It's a congenital disease with the abnormal growth, as we said before, of fibrous tissue and smooth muscle tissue. This entity can occur quite commonly in young women. Remember, the atherosclerotic form of renal artery stenosis is more common in women also because of the age factor. The commonest cause of renovascular hypertension among young patients is fibromuscular dysplasia. 05:32 There are degenerative diseases that affect the lining of the artery: the media (the smooth muscle) and the intima (the endothelium). There are multiple stenoses with intermittent dilation of the artery, and there can even be aneurysm formation in smaller branches of the renal artery. Let's talk a little bit about therapy of renovascular hypertension secondary to arterial stenosis. First-line therapy is medical therapy and lifestyle modification plus statins. If the cause of the renal artery stenosis is atherosclerosis, of course, always statins and all the lifestyle modifications we talked about: diet, stop smoking, control of blood pressure, and so forth. Often, this is enough to control the blood pressure in these patients. There are very specific medications that block the effect of renin that is released by the kidney, and we're going to talk about all of those things in the next lecture on hypertension. If medical therapy doesn't work very well, then one does stenting, just like in the coronary arteries: We open up the renal artery stenosis with a stent. And of course, then, in addition to the medical therapy we already talked about for the high blood pressure, you also have to give a platelet agent (for example, clopidogrel) to prevent a clot from forming in the stent. In very complex renal artery lesions, surgery is used, again, with a grafting—usually with a Dacron graft—just like we talked about with aortic aneurysms. The… If… In patients with fibromuscular dysplasia, of course, this is not due to atherosclerosis, so again, antihypertensive therapy and lifestyle modification. If the patient's obese, weight loss helps. And again, the angioplasty will often help here by opening up the renal artery. And again, in very complex patients you may need to go with surgery, and very often, these patients require antiplatelet therapy to prevent blood clotting in the repaired renal artery. Whether it's a stent or whether it's surgical, very often, you have to be on blood thinners to prevent clotting, which would, then, close the artery again. So in summary, we've talked about dissection
About the Lecture
The lecture Renal Stenosis and Fibromuscular Dysplasia by Joseph Alpert, MD is from the course Arterial Diseases.
Included Quiz Questions
What percentage of renal artery stenosis is due to atherosclerosis?
- 95%.
- 70%.
- 75%.
- 80%.
- 85%.
Goldblatt effect suggests constriction of renal artery causes secretion of which of the following substances?
- Renin.
- Angiotensin.
- ADH.
- Adrenaline.
- Erythropoietin.
Which age group is most likely to suffer from renal artery stenosis resulting from fibromuscular dysplasia?
- Young females
- Children
- Geriatric males
- Young males
- Preadolescent females
What percentage of renal stenosis is caused by fibro muscular dysplasia?
- 5%.
- 10%.
- 15%.
- 20%.
- 25%.
Author of lecture Renal Stenosis and Fibromuscular Dysplasia

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
