Playlist
Show Playlist
Hide Playlist
Projections of Viscera Onto the Back – Topographic Back Anatomy

-
Slides 04 Abdominal Wall Canby.pdf
-
Download Lecture Overview
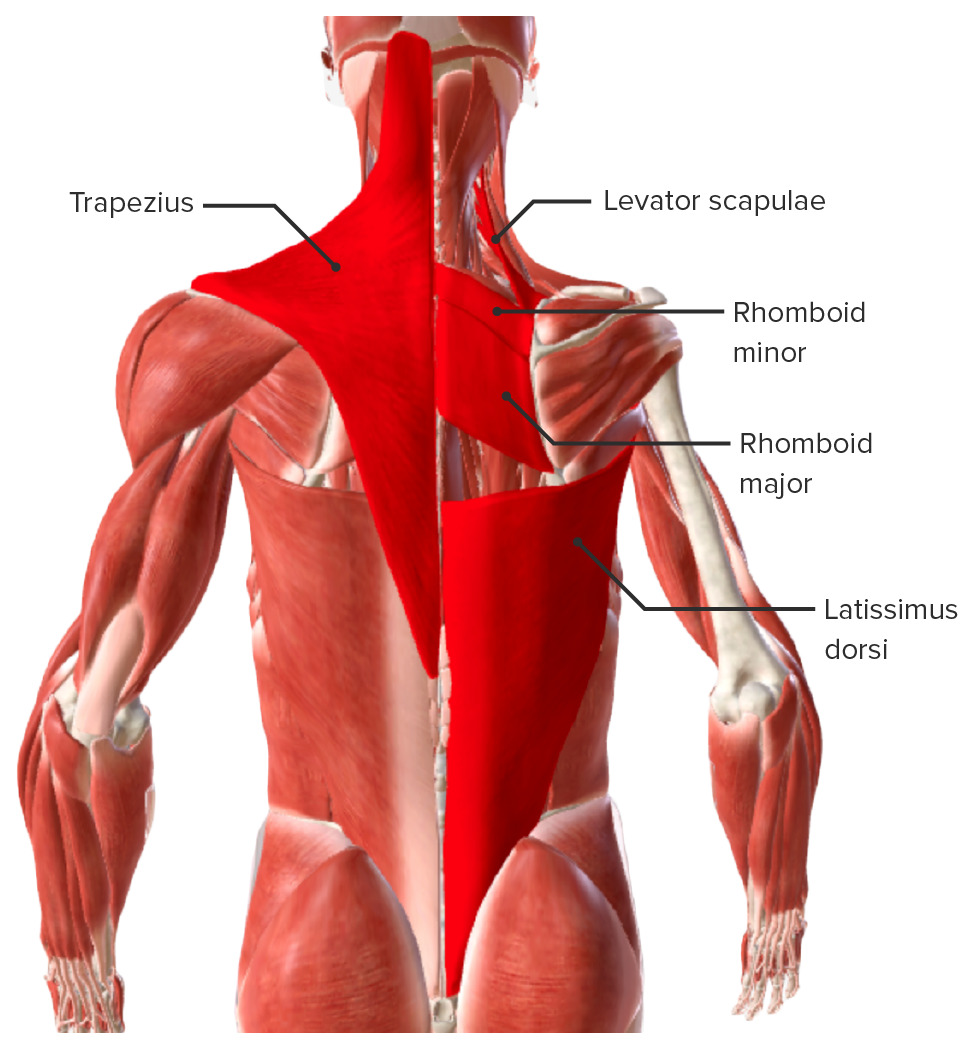
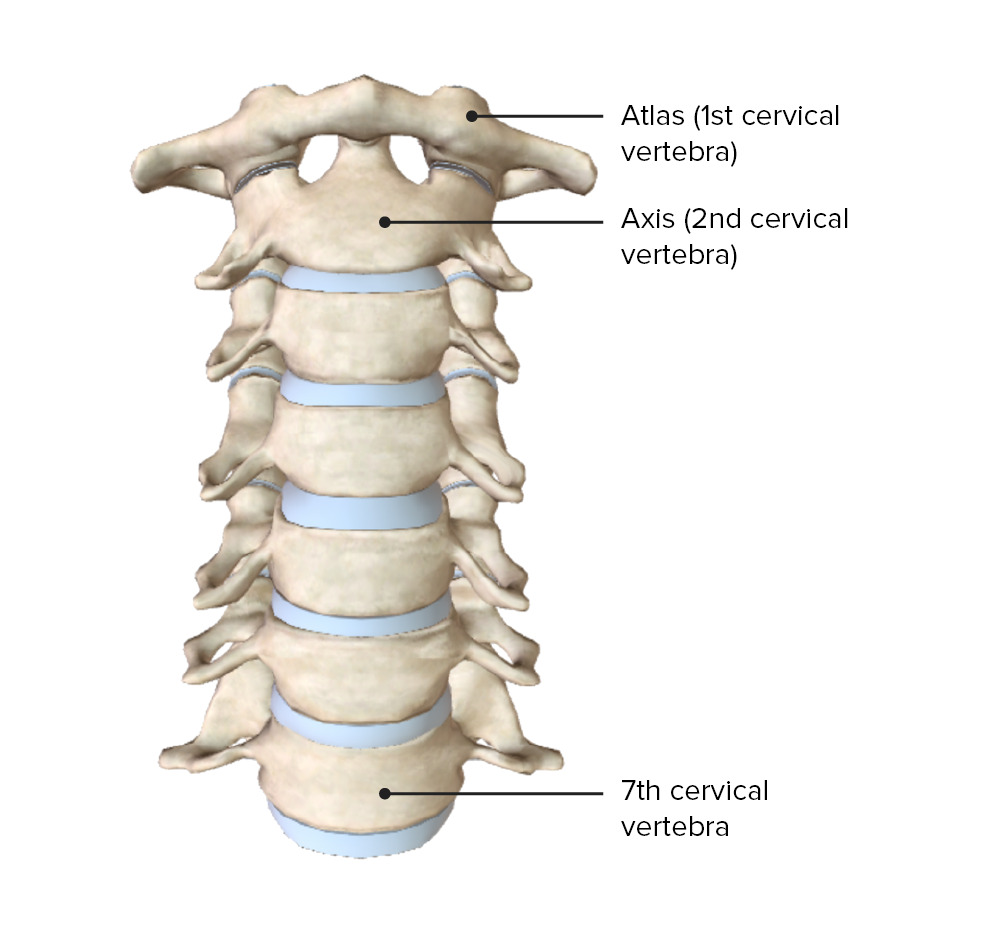
00:01 It’s also important to understand the projection of the lungs onto the back. This can be important clinically for doing something as simple as listening to the lungs, auscultation. And it’s also very, very useful in being able to perform a procedure referred to as a thoracentesis. So, what is this clinically relevant surface topography? Here we have a nice posterior view of the back. Our superior most area of interest is going to be the vertebra prominens again, C7. And as we take a look, the apex of the lung right in through here, it’s visceral pleura and then the dash line representing the parietal pleura is at the level of the vertebra prominens. 00:56 Inferiorly, the lung and the visceral pleura that’s adhered to it, has a rib relationship to the 10th rib. And then, if we look here more inferiorly, where we have the hash line, the hash line represents the inferior most limit of the parietal pleura. And then between the visceral pleura and the parietal pleura, we have a potential space, that’s referred to as the pleural cavity. We also have the spine of the scapula at this level. And so, if you want to listen to the lungs and you want to listen to the superior lobe versus the inferior lobe, you can use the spine as an important anatomic landmark. So, if you’re at the spine or above on either side, you can listen to lung sounds emanating from the superior lobes of either the right or left lungs. And then, if you come down well below the spine of the scapula here or here, you can then clearly listen to lung sounds that are emanating from the inferior lobes. It’s also useful in performing a procedure called the thoracentesis. Sometimes there’s excessive accumulation of fluid in the pleural cavities. 02:30 So, the potential space becomes a fluid-occupied space. And occasionally, this fluid may be due to blood accumulation. So, imagine this recess right in through here between the visceral pleura and the parietal pleura all of a sudden expanding with fluid. 02:52 The lung and its visceral pleura expands or gets pushes upward and then you have more and more fluid accumulating within the pleural space. By advancing a needle between the ribs where that fluid is located, you can then remove that fluid. And that procedure is a thoracentesis. 03:15 The posterior approach is superior in performing a thoracentesis procedure. Anatomically, the intercostal spaces are wider and the intercostal nerve bundle is closer to the inferior margin of rib. These anatomical considerations make this a safe space to enter the chest. The patient straddles a chair and leans forward on a pillow and the ideal intercostal spaces that maybe entered are the seventh, eighth or ninth midway between the posterior axillary line and midline of the back as these spaces avoid accidental puncture of organ, that is the liver, spleen diaphragm and aorta. A mid axillary approach may be also used for patients in a supine position, as the costodiaghragmatic recess is located between the ribs 8 and 10. The needle would be inserted over the superior border of the 9th rib and 10th rib, but not too far as to avoid injury of the liver if performed on the right, or spleen if performed on the left. Ultrasound guidance of this procedure decreases the risk of liver or spleen injury. Here we’re looking at the projection of kidneys onto the back and it’s important to understand that the superior most limits of both kidneys is a bit different because of the anatomic viscera that are present asymmetrically within the abdominal cavity. So, if we take a look at the two kidneys that are shown here, here’s your left kidney, here’s your right kidney. And you can see that the right kidney is pushed a little bit below the superior most aspect of the left kidney and that’s due to the presence of a large abdominal organ called the liver on the right and its presence on the left is not as huge. And so, the left kidney is able to have a more superior ascent than the right kidney. Ribs have relationships to these kidneys. 05:37 So, if we take a look at the left kidney, both the 11th rib and the last or 12th rib will have a relationship to the posterior aspect of the left kidney. However, on the right side, due to right kidney being a little bit below the left, only the 12th rib will have a posterior relationship to the right kidney. The kidneys and their vasculature do lie retroperitoneally. And so, it’s sometimes to one’s advantage, if there has to be a surgical approach to the kidney, to have a retroperitoneal approach. By doing so, the surgeon does not have to enter the peritoneal cavity, displace abdominal viscera and then cut through the parietal peritoneum that lines the anterior aspects of the kidneys. It’s interesting that in a retroperitoneal surgical approach, they’ll have to insufflate the retroperitoneal space with carbon dioxide, a gas. And the balloon and the catheter that’s utilized for this process and the subsequent process of introducing a dilating balloon catheter, you’re going to access the retroperitoneum by advancing the catheters through the inferior lumbar triangle that we defined in an earlier slide. 07:20 This slide represents the projection of other viscera onto the back. Here we’re looking at the spleen, the liver, duodenum, the pancreas as well as the large intestine. We do have two views that are depicted on this slide, an anterior view. But we really want to concentrate on the image to the right where we have a posterior view. And we’re going to concentrate more in the inferior aspect of the back where we have the presence of the liver. And you can see the superior most projection of the liver here. 08:02 Over to the left, we have the spleen and its surface topography onto the back well protected by the posterior aspects of the ribs at this level. Here is your kidney, the left kidney. 08:18 And then the 12th and 11th ribs relating to its posterior aspect. Again, your right kidney with the 12th rib is shown. Duodenum is seen in through here. And you can see the curved nature of the duodenum. We can also see the pancreas right in through here and it projects toward the spleen right in through here. Because of its relationship to the back and it being retroperitoneal, some individuals with pancreatic cancer, the first symptom is back pain. 09:02 And then we also have the surface projection of the large intestine. Here is the right-sided large intestine to include the appendix, caecum, ascending colon. This is a retroperitoneal structure on the right lateral aspect of the back. And then we have on the left side the descending colon, the sigmoid colon. That descending colon is also going to be retroperitoneal. 09:36 So, what are the take-home messages from this lecture? First, regions of the back are named according to their skeletal and muscular relationships. Muscles and skeletal elements provide surface relief to the back. The superior and inferior triangles are potential sites for herniation of abdominal contents. The intercristal lines are defined at lumbar vertebral level, which is clinically useful in performing a lumbar puncture. 10:17 Projections of the lungs onto the back is clinically useful in performing a thoracentesis. 10:25 Projections of the kidneys onto the back and inferior lumbar triangle are clinically useful in a retroperitoneal surgical approach to the kidneys. 10:36 And lastly, a pancreatic cancer commonly causes back pain. 10:42 Thank you for joining me on this lecture about the “Topography of the back”.
About the Lecture
The lecture Projections of Viscera Onto the Back – Topographic Back Anatomy by Craig Canby, PhD is from the course Abdominal Wall with Dr. Canby.
Included Quiz Questions
Which rib is related to the inferior-most portion of the lung along the paravertebral line?
- Rib 10
- Rib 4
- Rib 6
- Rib 8
- Rib 12
What is the procedure in which the inferior lumbar triangle is clinically useful?
- Retroperitoneal surgical approach to the kidney
- Thoracentesis
- Lumbar puncture
- Lung auscultation
- Heart auscultation
What is the potential space between the parietal pleura and the visceral pleura called?
- Pleural cavity
- Thoracic cavity
- Spinal cavity
- Abdominal cavity
- Pericardiac cavity
What is the surface landmark used to clinically differentiate between the superior and inferior lobes of the lung?
- Spine of scapula
- Clavicle
- Inferior border of scapula
- Right border of scapula
- Left border of scapula
Which ribs are related to the posterior surface of the left kidney?
- Ribs 11 and 12
- Ribs 9 and 10
- Ribs 8 and 9
- Ribs 6 and 7
- Ribs 10 and 11
Author of lecture Projections of Viscera Onto the Back – Topographic Back Anatomy

Craig Canby, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
