Playlist
Show Playlist
Hide Playlist
Pneumothorax: Diagnosis in Radiology

-
Slides Pneumothorax.pdf
-
Download Lecture Overview
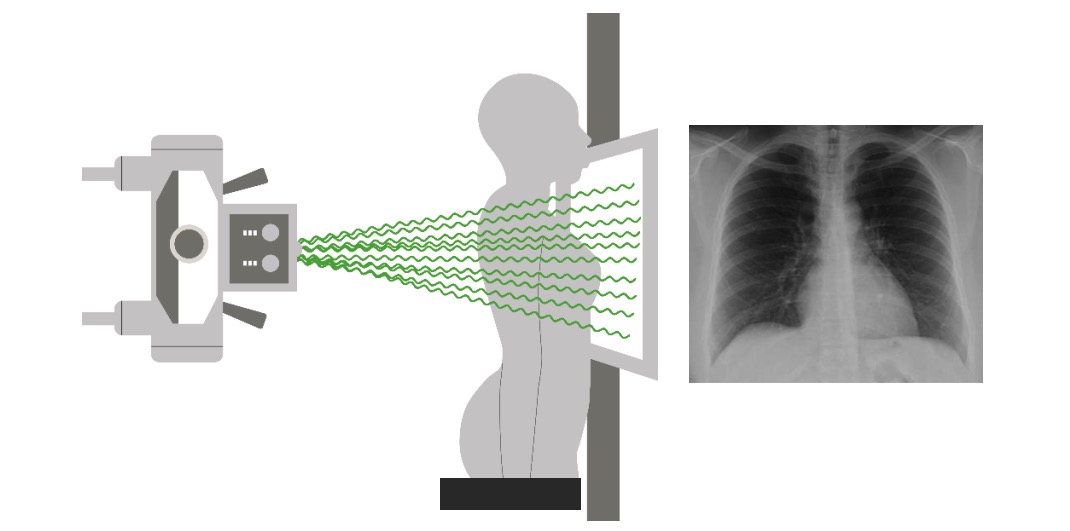
00:01 So, what's the best way of diagnosing a Pneumothorax? When a patient comes in and you're suspecting a pneumothorax then upright chest radiograph is really the fastest method and it has very good sensitivity. 00:11 But what can you do if the patient can't be upright, is there another alternative? So, these are the three different alternatives that you have. 00:24 You could perform an expiratory chest radiograph, remember that most chest radiographs are performed in the inspiratory phase because you want to expand the lungs as much as possible to take a good look at what's going on. 00:34 You can also perform a decubitus radiograph, or you can perform a CT. 00:40 So the expiratory radiograph will actually decrease the amount of air that's in the lung which decreases the lung's size. 00:46 When the lung size decreases, the size of the pneumothorax will remain unchanged and that makes it more visible. 00:52 On a decubitus radiograph, again, air rises to the highest point and this is due to gravity, so the patient should actually be placed with a suspected pneumothorax side up and that will raise the pneumothorax up to the top and you can see it well. 01:09 A CT as we saw, is very sensitive in the diagnosis of a pneumothorax. 01:14 So this is an example of a decubitus film. 01:17 This patient is lying on their right side so if you're suspecting a left-sided pneumothorax, this would be a good position. 01:23 The air would rise to the top of the patient and you can see it well. 01:27 CT as we saw is highly sensitive but it is more expensive and it's actually time-consuming, so you don't wanna start off with that unless you absolutely have to. 01:36 So, two of the things that are very commonly confused are a pneumothorax versus atelectasis. 01:45 Both are a collapse of the lung and that makes it a little bit confusing when people are learning the differences between the two. 01:51 So a pneumothorax actually results in air between the visceral and the parietal pleura which then separate. 01:58 Atelectasis is collapse of the lung but the visceral and the parietal pleura remain attached and so that's really the big difference between the two. 02:06 In a pneumothorax, structures shift away from the pneumothorax because you have increased pressure in the pleural space and that pushes the visceral pleura and the lung away. 02:15 In atelectasis however, you actually have shift towards the side of the atelectasis because you have lack of pressure within the collapsed lung and since the visceral and the parietal pleura are still attached, they get pulled towards the collapsed lung. 02:29 A pneumothorax appears dark and you see that thin visceral line that we discussed. In atelectasis, the area actually appears white. 02:36 So they appear very different and they have a different pathological basis but they can be confusing because they're both called lung collapse. 02:44 So we've gone over some common findings associated with a pneumothorax. 02:49 Again, this is a finding that you really don't want to miss because when it gets large, it can lead to hemodynamic collapse.
About the Lecture
The lecture Pneumothorax: Diagnosis in Radiology by Hetal Verma, MD is from the course Thoracic Radiology. It contains the following chapters:
- Pneumothorax Diagnosis
- Pneumothorax vs. Atelectasis
Included Quiz Questions
Which of the following imaging studies will NOT be helpful to diagnose a right-sided pneumothorax?
- Right lateral decubitus chest radiograph
- PA Chest radiograph
- CT
- Left lateral decubitus chest radiograph
- Expiratory chest radiograph
Which of the following statements is helpful to differentiate pneumothorax from atelectasis?
- In pneumothorax, the structure may shift to the opposite side of the pneumothorax.
- In atelectasis, increased pressure in the pleural space pushes the visceral pleura and the lung away.
- The chest X-ray in atelectasis appears dark.
- In pneumothorax, the visceral and parietal pleura remain attached.
- In pneumothorax and atelectasis structures may shift towards the same side.
Author of lecture Pneumothorax: Diagnosis in Radiology

Hetal Verma, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Really well explained. use of the chest X-rays where we pause and try to work it out is really good
