Playlist
Show Playlist
Hide Playlist
Klinefelter (XXY) and Turner Syndrome (Gonadal Dysgenesis)


-
Slides KlinefelterandTurnerSyndrome Pediatrics.pdf
-
Download Lecture Overview
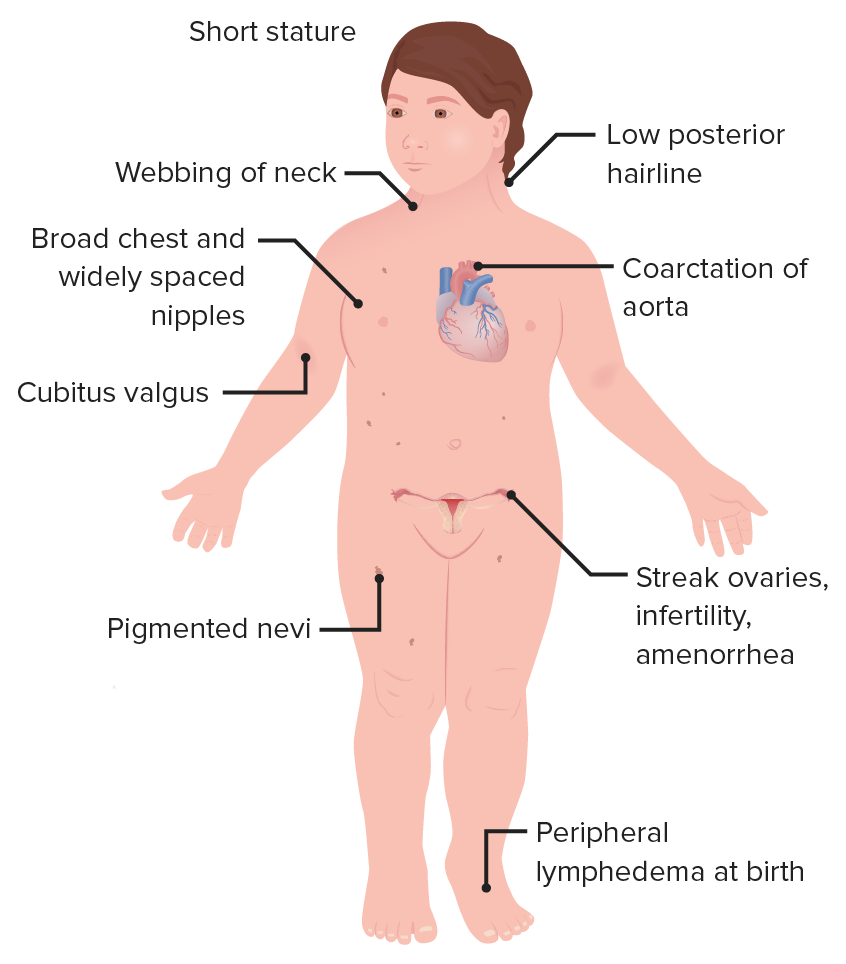
00:01 In this lecture, we will discuss Klinefelter Syndrome and Turner Syndrome. 00:06 These are genetic problems with the sex chromosomes. 00:09 So let?s start with Klinefelter Syndrome. 00:12 These patients usually have male hypogonadism. 00:15 They have 2 or more X chromosomes and 1 or more Y chromosomes. 00:20 Most commonly, two X?s and one Y like you can see in this patient?s karyotype. 00:25 This occurs in 1 out of 650 live births. 00:29 So, it?s not that uncommon. 00:30 This is generally due to maternal or paternal nondisjunction during meiosis as they?re making either the sperm or the egg. 00:38 There?s a slightly increased risk of this happening in mothers who are of advanced maternal age. 00:46 Sometimes, Klinefelter Syndrome patients are fertile and can go on to have their own children. 00:54 Fertile Klinefelter Syndrome patients have a low reccurence of Klinefelter Syndrome in their offspring, but the offspring do carry a very small increased risk of chromosomal abnormalities. 01:06 So let?s review the clinical features of Klinefelter Syndrome. 01:11 They often suffer infertility. 01:14 They may have hypogonadism with small testes. 01:18 They often have gynecomastia in adolescence as a result of an imbalance between testosterone and estrogens. 01:26 You?ll notice they have reduced body hair. 01:29 They will be tall and have a ?pear shaped? stature to them and they occasionally have educational and psychological problems. 01:39 So how do we diagnose Klinefelter Syndrome if we suspect the patient might have it? Well first, we?ll send a karyotype or an array comparative genomic hybridization. 01:51 This will make our definitive diagnosis. 01:53 We will also screen these patients when they are adult males for infertility. 01:58 That?s useful for them to know about for often they a decreased sperm count. 02:03 It?s important to check their testosterone levels. 02:06 They will often have a decreased testosterone in the phase of hypergonadotropism. 02:12 In other words, they have hypergonadotropic hypergonadism. 02:17 Their testes are nonresponsive to LH and FSH, so they have high LH and FSH hormone levels. 02:25 So how do we improve these patients? lives? The first thing that?s very important is that they should receive testosterone therapy. 02:35 This will help a number of things especially their facial and body hair issues. 02:40 It will improve their strength and muscle size. 02:42 It will improve their energy level. It will help them with libido issues. 02:46 It will help them with confidence and it will help them with concentration. 02:51 So we often will refer these patients to reproductive specialists or infertility specialists as well to help them with various reproductive options if they should decide to have a child. 03:03 So let?s focus now on Turner Syndrome. 03:06 Turner Syndrome is a partial or a complete monosomy of the X chromosome. 03:12 This results in hypogonadism in the phenotypic female. 03:17 The incidence is about 1 in 2,000 live births. 03:21 So how does this happen? Well, more than 60% are due to do novo meiotic nondisjunction in the paternal sex chromosomes. 03:32 So the dad has an X and a Y and instead of splitting into one X and one Y sperm is basically an XY sperm and an empty sperm and the empty sperm now then goes and fertilizes the egg creating a single X chromosome. 03:47 Turner Syndrome occurs essentially only in females. 03:51 Males can be mosaic for Turner Syndrome. 03:56 This is rare but it can happen where a male has some cells that are 45, X and other cells that are 46, XY. 04:05 So what are the symptoms in females of Turner Syndrome? These are important to remember. 04:12 These patients will have a delayed puberty. 04:15 They will often have amenorrhea. This is from gonadal dysfunction. 04:20 They may have premature ovarian failure. 04:23 This results in infertility and some patients may have some learning disabilities especially in Math but generally, these patients are cognitively normal. 04:35 Patients with Turner Syndrome may have short stature. 04:40 In fact, they almost always do. 04:41 They have low set ears, a low hairline and you may notice a webbed neck or a broadened neck root. 04:49 Additionally, you can see small jaw, a ?shield chest? which is a broadened or a widened chest often with widely spaced nipples. 04:59 You may see cubitus valgus or outward-turned forearms. 05:04 They may have a horseshoe kidney internally which they may not even know about and they can develop congenital heart disease. 05:11 So how do we test and when do we test for Turner Syndrome? You should consider attempting prenatal diagnosis if the fetal ultrasound shows intrauterine growth restriction, fetal edema, a coarctation of the aorta or cystic hygroma. 05:30 In this case, if a parent wishes to do a prenatal testing, we generally do chorionic villi sampling or amniocentesis with karyotype. 05:39 Postnatally, the diagnosis is made by karyotype or aCGH just like in Klinefelter Syndrome. 05:48 So what therapy do we provide these patients? After initially making the diagnosis, we will screen them generally with an echocardiogram or a renal ultrasound especially paying attention to any abnormalities of the heart such as aortic problems or if there?s an abnormal kidney. 06:09 Additionally, we will typically check them for their thyroid function. 06:13 We?ll do an eye exam and we will assess for scoliosis which is a little bit more common in these patients. 06:19 It?s important to refer these patients to a pediatric endocrinologist for hormonal replacement. 06:25 These patients will receive estrogen, progestin and growth hormone. 06:30 If you look at this picture, here are two patients with Turner Syndrome. 06:35 The one on the left received no growth hormone and the one on the right received growth hormone. 06:42 Growth hormone is indicated in these patients and can really help them in terms of achieving an important stature. 06:48 The reason why we give it is because for patients who don?t achieve 5 feet of height, this can result in significant impairment and their ability to function in the world and may be simply hard for them to drive a car. 07:01 We want these patients to live the most fulfilled life that they can. 07:05 It?s also important to refer these patients to fertility specialists for consideration of their reproductive options when they enter into adulthood. 07:14 So that?s my review of Turner Syndrome and Klinefelter Syndrome. 07:18 Thanks for your time.
About the Lecture
The lecture Klinefelter (XXY) and Turner Syndrome (Gonadal Dysgenesis) by Brian Alverson, MD is from the course Pediatric Genetics. It contains the following chapters:
- Klinefelter Syndrome
- Turner Syndrome
Included Quiz Questions
Which of the following medications is most appropriate for patients with Turner syndrome?
- Growth hormone
- Beta blockers
- Alpha-2 antagonists
- Stimulants
- Oxytocin
Which of the following is the characteristic finding in Klinefelter syndrome?
- Hypergonadotropic hypogonadism
- Hypogonadotropic hypergonadism
- Hypogonadotropic hypogonadism
- Hypergonadotropic hypergonadism
Karyotyping in a 12-year-old boy reveals 47, XXY. Which of the following is the most appropriate pharmacotherapy in this patient?
- Testosterone
- Progesterone
- Estradiol
- Levothyroxine
- Gonadotropins
Which of the following is not true regarding patients with Turner syndrome?
- They are phenotypically male.
- They have delayed puberty.
- They develop premature ovarian failure.
- Some inherit a missing paternal sex chromosome
- Most are genotypically female.
Which of the following findings is not typical of a patient with Turner syndrome?
- Tall stature
- Webbed broad neck
- Horseshoe kidneys
- Cubitus valgus
- Congenital heart disease
Which of the following prenatal findings suggests Turner syndrome and a need for prenatal karyotyping?
- Cystic hygroma
- Large for gestational age
- Polydactyly
- Long femur
- Lung hypoplasia
Which of the following findings is not true regarding patients with Klinefelter syndrome?
- They are genotypically female.
- They are phenotypically male.
- They have reduced body hair.
- They have hypogonadism.
- They are tall.
Author of lecture Klinefelter (XXY) and Turner Syndrome (Gonadal Dysgenesis)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
