Playlist
Show Playlist
Hide Playlist
Introduction to Motor Neurons and Motor/Sensory Pathways

-
Slides Diseases of the Motor Neurons.pdf
-
Download Lecture Overview
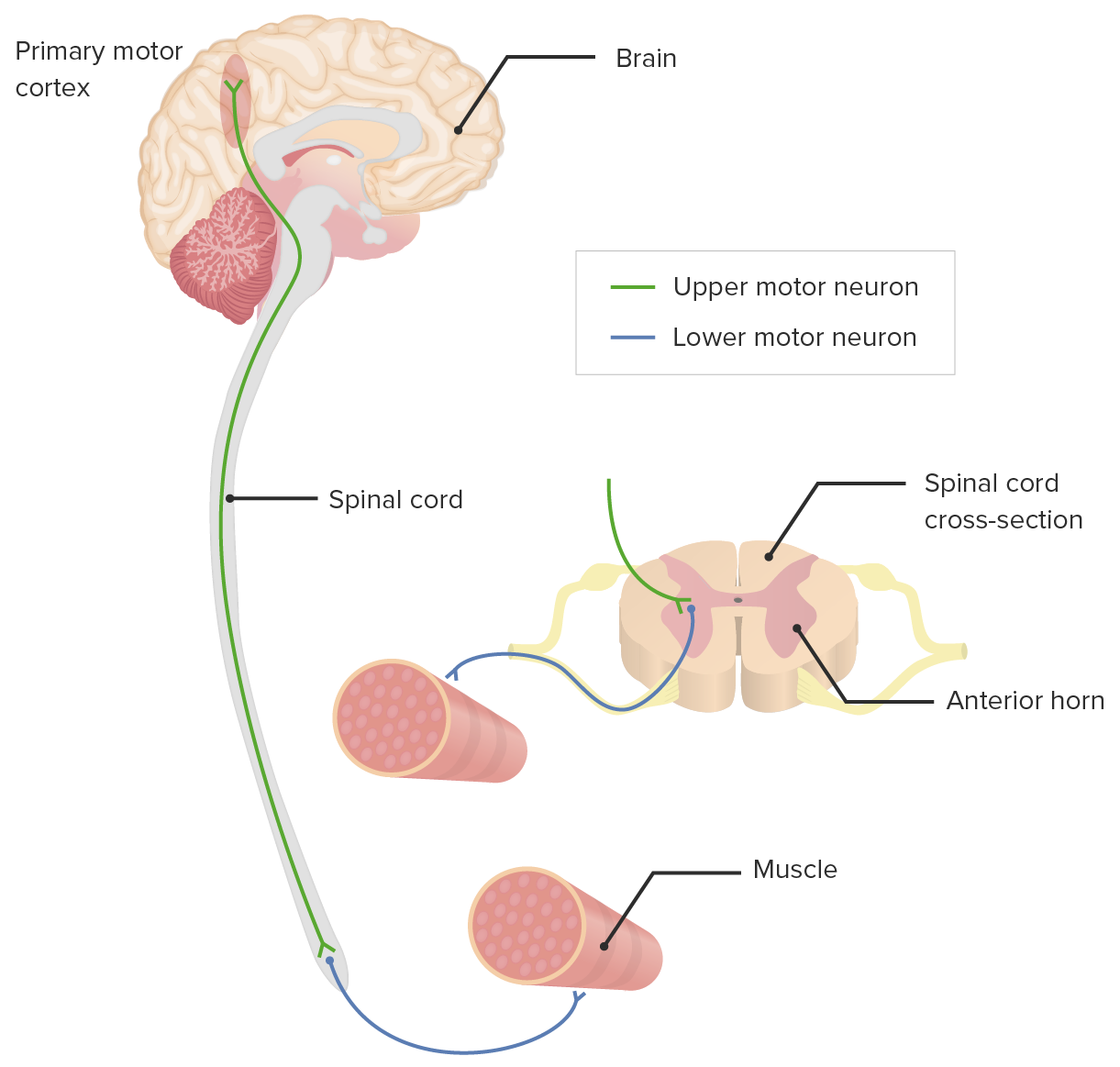
00:01 Let's start back at some basic anatomy. 00:04 And here we see a schematic of the brain. 00:06 We're looking at the lateral aspect, a lateral view of the brain, and we see the central sulcus with the precentral gyrus and the post central gyrus. 00:14 The central sulcus divides the motor lobe, which is the frontal lobe from the sensory lobe, which is the parietal lobe. 00:20 And that precentral gyrus is the motor cortex and the motor gyrus is the primary motor cortex or Broddman's area 4. 00:29 This contains the primary motor cortex and the neurons involved in volitional motor control. 00:35 It also contains the large neurons known as the Betz cells and those Betz cells are really the generator, they are the cells of origin of those first order upper motor neurons. 00:46 That's where the motor neurons start and then descend down into the spinal cord and the Betz cells are important. 00:52 They are the ones that degenerate in motor neuron disorders like ALS. 00:58 The primary motor cortex controls voluntary movement and so patients present with weakness with voluntary muscle muscle groups and not those autonomic innervations of motor function. 01:15 So let's dive a little bit more into motor neuron anatomy and follow the course of the primary motor neuron from the cortex down to the spinal cord. 01:25 The upper motor neurons begin and the Betz cells in the precentral gyrus of the primary motor cortex and we can see here the homunculus of the primary motor cortex, upper motor neurons or cell bodies in the motor cortex. 01:39 Their axons descend ipsilaterally via the internal capsule and descend into the spinal cord. 01:46 And in the spinal cord, the primary motor neurons connect with the lower motor neurons in the cell bodies of the ventral horns. 01:55 Here we can see the descension of the first order motor neuron, the upper motor neuron from the primary motor cortex down into the internal capsule to the cerebral peduncles, decussating at the pyramids, descending in the lateral corticospinal tract, and then terminating in the ventral horn of the spinal cord segment that will give rise to the lower motor neuron at the segment that is innervated. 02:21 Now let's turn to the lower motor neuron. 02:23 What's the course of the lower motor neuron? Where does it arise and where does it go? Lower motor neurons are the efferent neurons in the peripheral nervous system. 02:30 They connect the central nervous system with the muscles that allow voluntary motor movement. 02:36 The cell bodies of the lower motor neuron are located in the anterior horn, the ventral horn of the spinal cord. 02:42 And the axons terminate in the neuromuscular junction of the respective muscle traveling in the peripheral motor nerve. 02:51 So now let's talk a little bit about the localization and somatotopy of the motor neurons. 02:55 We can better understand how patients present the symptoms that develop in patients with motor neuron disease and how we're going to diagnose that. 03:03 First of all, what controls voluntary motor movement? Well, it's the corticospinal tract. 03:10 And the corticospinal tract is one of the key parts of the pyramidal system. 03:15 That pyramidal system controls volitional motor control. 03:18 And that's different from some of the automatic control of movement, which may be coming from the extrapyramidal system managed by the basal ganglia. 03:27 When we think about the upper motor neuron pathways, we think about corticobulbar tracts and corticospinal tracts. 03:34 The corticobulbar tract connects the cerebral cortex to the nuclei of the cranial nerves in the brainstem and that controls the muscles that move the face. 03:43 The corticospinal tracts connects the cerebral cortex to lower motor neurons and interneurons in the spinal cord and this is the tract that descends into the cord and controls all of the body's volitional movements. 03:55 There are two corticospinal tracts - the lateral corticospinal tract, which contains 85% of the motor fibers from the primary motor cortex. 04:04 These cross or decussate in the caudal medulla at the pyramidal decussation and descend to the level of the spinal cord, where they synapse with the peripheral nerve, the peripheral motor nerve. 04:15 15% of those motor fibers actually continue to descend and not decussate and descend in the anterior corticospinal tract, which as you can see here contains approximately 15% of the motor fibers. 04:27 They crossed at the same level of the spine as they innervate. 04:32 So let's look closer at that motor pathway. 04:35 Again, motor neurons arise at the precentral gyrus, descend in the internal capsule through the midbrain, pons, medulla of the brainstem decussate at the pyramids and you can see that here. 04:48 Here we're looking at the corticobulbar tract which again begins in the motor cortex and descends where it innervates the cranial nerve nuclei in the brainstem. 04:57 The corticospinal tract, 85% decussates at the level of the pyramids and descends in the lateral corticospinal tract and that 15% remains ipsilateral to its cell body of origin in the anterior corticospinal tract. 05:10 And this gives rise to central nervous system control of volitional movement, it's how we move Those primary motor neurons then descend into the ventral gray matter of the spinal cord, and synapse with lower motor neurons that travel out to the muscles, the distal muscles involved in fine movement, the proximal muscle involved in gross movement, and so disorders that affect the lower motor neurons will affect both distal fine and proximal gross movements. 05:41 When we think about the somatotopy of the spinal cord itself, there are both sensory and motor tracts present in the spinal cord and you can see those here, we've labeled them with the with the regions of the body that are innervated S is sacrum, L - lumbar T - thoracic and C - cervical and you can see in general, the sacral and lumbar regions are contained in the outer parts of the spinal cord and the cervical, and cervical and thoracic regions are contained in the inner parts of the spinal cord. 06:09 And this is important in looking at evaluating spinal cord pathology. 06:14 Central lesions to the cord will result in sacral sparing, will have involvement of the cervical regions and some patients present with a cape-like distribution of abnormal findings with sacral sparing. 06:27 And that is contrasted with externally compressive processes, which spares the cervical fibers and begins with the lower lumbosacral fibers and disorders affecting those fibers first.
About the Lecture
The lecture Introduction to Motor Neurons and Motor/Sensory Pathways by Roy Strowd, MD is from the course Diseases of the Motor Neurons.
Included Quiz Questions
Which of the following are paired correctly?
- Primary motor cortex ‒ neurons involved in volitional motor control
- Upper motor neurons ‒ synapse at the neuromuscular junction
- Lower motor neurons ‒ Betz cells
- Primary motor cortex ‒ parietal lobe
- Upper motor neurons ‒ cross to the contralateral side in the internal capsule
Which best describes the pathway that the majority of upper motor neurons course through to synapse with lower motor neurons?
- Primary motor cortex → ipsilateral internal capsule → ipsilateral cerebral peduncle → pyramidal decussation → contralateral lateral corticospinal tract and ventral horn
- Primary motor cortex → decussate at the internal capsule → ipsilateral cerebral peduncle → contralateral pyramid → contralateral lateral corticospinal tract and ventral horn
- Primary motor cortex → ipsilateral internal capsule → ipsilateral cerebral peduncle → ipsilateral pyramid → ipsilateral corticospinal tract → decussate at the ventral horns of the spinal cord
- Primary motor cortex → ipsilateral internal capsule → decussate at the cerebral peduncles → contralateral pyramid → contralateral lateral corticospinal tract and ventral horn
A central cord lesion is most likely to spare nerve fibers in which region?
- Sacral
- Cervical
- Lumbar
- Thoracic
Author of lecture Introduction to Motor Neurons and Motor/Sensory Pathways

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
