Playlist
Show Playlist
Hide Playlist
Hyponatremia and Its Neurologic Effects

-
Slides Water Balance Hypo and Hypernatremia.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
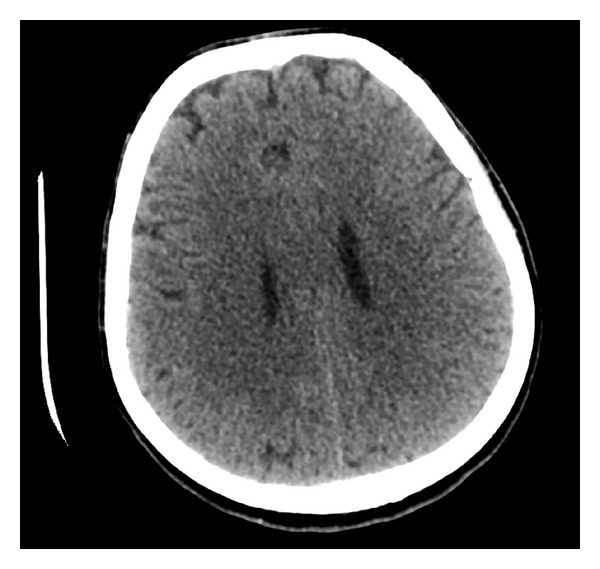
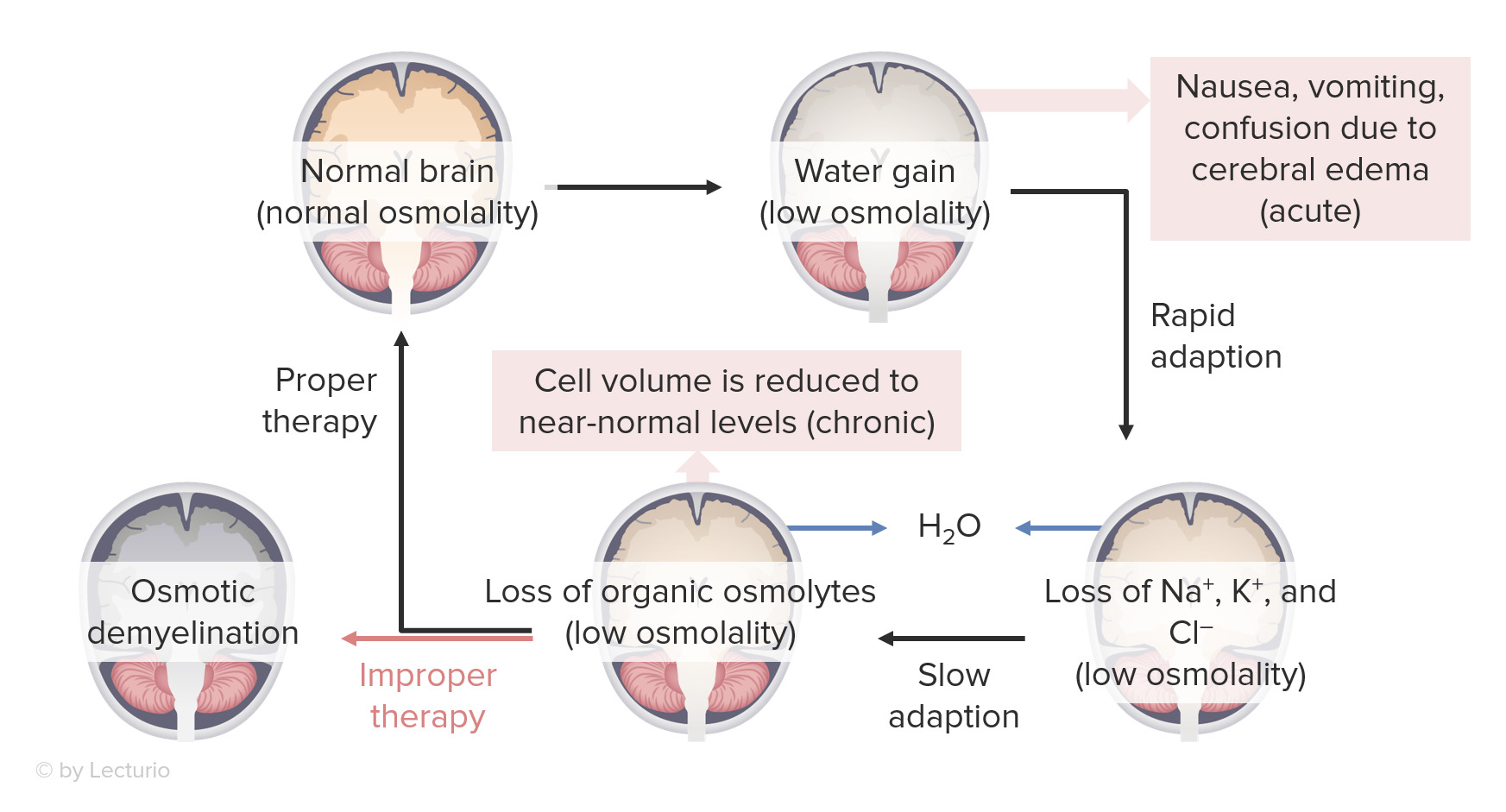
00:01 So before we move on to talk about the clinical entities of hypo and hypernatremia, it's very important to understand some clinical terms when we evaluate patients who have problems with water balance. 00:12 So one thing and a concept that you need to understand is that sodium. 00:16 That's that primary cation in the ECF. 00:19 That is what determines our extracellular fluid volume. 00:23 So a patient who has hypovolemic, meaning that their volume depleted has a total body sodium deficit. 00:31 A patient on the other hand, who is hypervolemic is volume overloaded. 00:36 They have an excess total body sodium. 00:39 Now, that's not measured by their serum sodium. 00:42 This is measured by their physical exam. 00:45 If a patient is hypovolemic, they'll have a low blood pressure. 00:48 If a patient is hypervolemic, they might have elevated neck veins or signs of edema. 00:55 A patient who is euvolemic means that they are normovolemic or they have normal volume. 01:01 So they have a normal total body sodium. 01:06 Now, when we talk about hydration, Hydration impacts cell volume. 01:10 So, if a patient is over hydrated, that means that they have water intoxication. 01:17 And remember two thirds of that water is going to move to the intracellular compartment, so they have cell swelling. 01:22 When a patient is dehydrated, that means they are water depleted, and then cells will shrink. 01:31 So, now that we've got those concepts underway, let's start talking about how patients will clinically present when they have problems with water balance like hyponatremia. 01:42 Hyponatremia is defined as a serum sodium of less than 135 mEq/L. 01:47 And it results from intake and subsequent retention of water. 01:52 So they have water excess in most situations. 01:57 Also, patients will have an impairment in renal water excretion. 02:02 So when a patient is hyponatremic during hospitalization, that's actually a significant prognostic issue and portends a bad prognosis. 02:11 About 2.5% of hospitalized patients present with hyponatremia. 02:15 But two-thirds of those are acquired during the hospitalization. 02:19 Now, mortality is actually increased 60-fold in patients who are hyponatremic. 02:24 It probably is a marker rather than a cause. 02:29 About 90% of hospitalized patients who are hyponatremic due to nonosmotic release of ADH. 02:38 So when we think about the effects and clinical manifestations of hyponatremia, what we worry about is what happens neurologically. 02:46 So remember, if we have an increase in total body water, then two-thirds of that is going to go to the intracellular compartment. 02:53 And that's fine for most entities in our body, but think about our brain. 02:58 Our brain and our neuronal cells are actually enclosed in a rigid calvarium. 03:03 So if we have water intoxication, then those cells will start to swell within our rigid calvarium and can cause cerebral edema. 03:11 The earliest manifestations patients will start to feel nauseated, they may vomit, they have confusion, and this is because of acute cerebral edema. 03:21 Now, our body is being as elegant as they are have an autoregulatory process where they have a rapid adaptation. 03:28 And what will happen is in the neuronal cells, we will lose sodium, and potassium, and chloride. 03:34 Those ions will move from the intracellular compartment to the extracellular compartment. And what happens? Water follows. 03:41 So it brings that cell volume back to normal. 03:46 If this is sustained over a 48-hour period of time or longer, then we start to move organic osmolytes from the intracellular compartment to the extracellular compartment. 03:55 Again, water is going to follow and then our cell volume goes back to normal. 04:00 So we could chronically adapt to this excess water.
About the Lecture
The lecture Hyponatremia and Its Neurologic Effects by Amy Sussman, MD is from the course Water Balance: Hypo- and Hypernatremia.
Included Quiz Questions
Which of the following would one expect in a hypovolemic patient?
- Total body Na+ deficit
- Total body Na+ excess
- Total body free water excess
- Total body K+ excess
- Total body K+ deficit
Which of the following is the most common cause of hyponatremia in hospitalized patients?
- Nonosmotic release of ADH
- Excessive activation of the renin-angiotensin-aldosterone system
- Inappropriate intravenous fluid therapy
- Increased release of ANP-related peptides
- False-positive laboratory test results
How does the brain adapt to acute cerebral edema caused by hyponatremia?
- By transporting Na, K, and Cl from the intracellular compartment to the extracellular compartment
- By transporting Na, K, and Cl from the extracellular compartment to the intracellular compartment
- By increasing CSF production
- By transporting urea from the extracellular compartment to the intracellular compartment
- By transporting urea from the intracellular compartment to the extracellular compartment
Author of lecture Hyponatremia and Its Neurologic Effects

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
