Playlist
Show Playlist
Hide Playlist
Diuretics – Hypertension

-
Slides 07 Cardiology Alpert EN.pdf
-
Reference List Cardiology.pdf
-
Download Lecture Overview
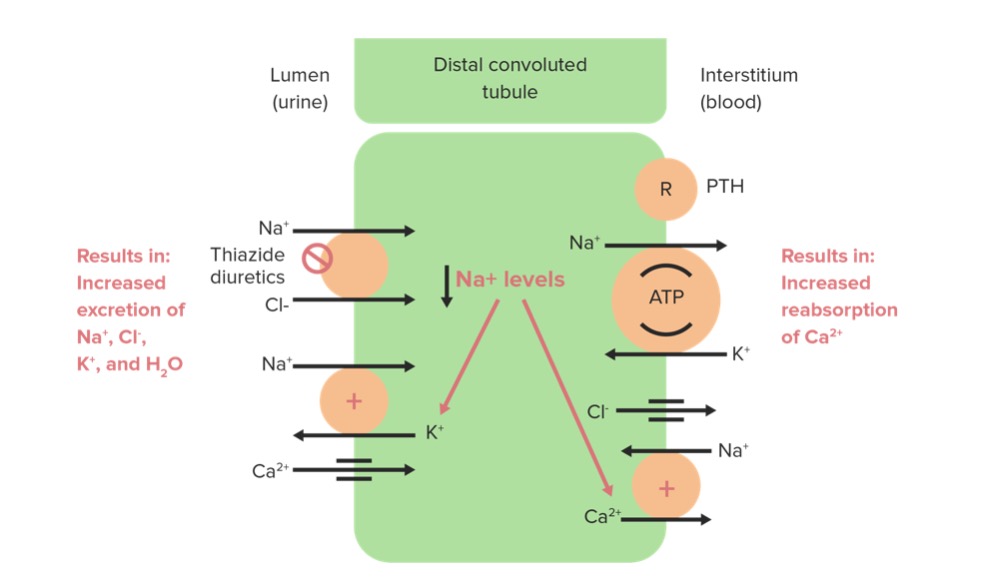
00:00 So, first let’s talk about first line diuretics. 00:03 As you can imagine, there have been a lot of randomized double-blind controlled trials testing different drugs for control of hypertension. I’m going to only tell you about the ones where there’s excellent data that says, “These drugs really work.” Not only do they decrease blood pressure, but they also decrease the risk for stroke and for heart attack and kidney failure and all the things we talked about before that are the end result of uncontrolled high blood pressure. This little diagram is a diagram of the… of course, multiple times magnified of the kidney tubule system that makes urine. It turns out that diuretics or drugs that increase urine flow are also anti-hypertensive. And there are three different categories of diuretic, but the one that works best for controlling blood pressure is the one that works in the distal tubule of the kidney, the Thiazide diuretics. So, Thiazide diuretics have been known for decades to be very excellent in controlling blood pressure. They're generic, they're very inexpensive and they're usually very, very well tolerated. They increase urine flow a little bit, not a huge amount, but they also have effects on the blood vessels so that they decrease peripheral resistance and thereby, they drop the blood pressure. 01:29 There are a number of Thiazide diuretics, and again, as I said, doctors will decide, “Oh, this is the one I like best because my patients tolerate it best, there’s less side effects or it’s less expensive, it’s easier to get.” The one that I use, as you can see down there, the one that says HCTZ, that stands for hydrochlorothiazide. And the pharmacist know when I write a prescription for HCTZ that that’s what we’re getting. 01:54 Chlorthalidone is another one that’s quite popular. It’s actually a little more effective at lowering blood pressure compared to hydrochlorothiazide, but has more side effects. And here’s a little data from a scientific study in which patients who are on hydrochlorothiazide with reasonable control of blood pressure were switched to chlorthalidone and what you see from the left to the right is that when they switch to chlorthalidone, their blood pressure was lower. Unfortunately, the side effects were also more increased, particularly, low blood potassium. Potassium is an essential mineral in our blood. 02:29 It determines a good muscle function, good nerve function, a whole variety of important biochemical functions relate to having a good potassium level. When your potassium level is low, you may have cramps and fatigue and actually, you may even have electrical short circuits in the heart - arrhythmias. So, we try not to have people have low potassium and that’s one of the problems with chlorthalidone. It lowers potassium more than hydrochlorothiazide. 03:00 Hypokalemia or low potassium is one of the commonest side effects with diuretics. Why? Because the diuretics cause potassium to be washed out in the urine. So, for that reason, I don’t usually use chlorthalidone. I usually use hydrochlorothiazide and I try and use the smallest dose possible so I decrease the risk for high… for hypokalemia and the high risk kinds of complications that occur with hypokalemia. 03:30 As you see here, the risk of the problems with hypokalemia, it’s dose related. So, I try and give the smallest dose tolerated that controls the blood pressure and that gets me good control of the blood pressure without a lot of side effects. 03:48 Another side effect from thiazides is that they have a tendency to push people towards diabetes. So, if you are an inherited person where lots of folks in your family, you have an inheritance for diabetes, lots of family members with diabetes, of course, thiazide diuretic might not be the best choice for you because it might push you into having overt or clinical of diabetes. And if you have a tendency towards gout, thiazide diuretics can cause gout too. So, when we talk to the patients, we usually want to find out, do they have any of these risks. Have they had problems with hypokalemia in the past with other drugs, are there a lot of diabetics in their family, have they had gout or lots of family members with gout? Thiazides wouldn’t be the first choice in somebody who had one of these kinds of complications. And if there’s kidney damages ahead of time, we usually don’t use diuretics because they can worsen the kidney damage. 04:41 Now, there’s a complex series of actions from the different kinds of blood pressure medicines and what this diagram shows you is that some of the medicines, on the arrow on the left hand side, decrease peripheral vascular resistance. The thiazides do that, I just mentioned that. On the other hand, drugs that I’ve mentioned before in the arena of ischemic heart disease, Beta Blockers decrease the cardiac output and decrease the heart rate and they drop the blood pressure in that fashion. And then, there are drugs that actually quiet down the ‘oomph’ of the heartbeat, the contractility of the heartbeat, Beta Blockers can do that and some calcium blockers do that. And that also decreases the blood pressure. And by the way, as you’ll find out later in this lecture, it usually requires more than one drug to control blood pressure. Very few people are controlled with one drug. So, you often use a combination. You might use a combination of a thiazide to decrease peripheral vascular resistance and, for example, a Beta Blocker in order to decrease the cardiac output a little bit, or other combinations. And we’ll talk a little bit about the favorite combinations in a moment.
About the Lecture
The lecture Diuretics – Hypertension by Joseph Alpert, MD is from the course Cardiac Diseases.
Included Quiz Questions
Which of the following is the primary site of action of thiazide diuretics?
- Distal convoluted tubule of the kidney
- Ascending loop of henle
- Descending loop of henle
- Collecting duct
- Renal artery
Which of the following is a known adverse effect of thiazide diuretics?
- Glucose intolerance
- Migratory polyarthritis
- Metallic taste
- Peptic ulcers
- Blurred vision
Which one of the following is a relative contraindication to thiazide use?
- Gout
- Anemia
- Hyperkalemia
- Polycythemia vera
- Basal cell carcinoma
Reduction in blood pressure can be achieved by reducing peripheral vascular resistance. Which of the following medications work by reducing peripheral vascular resistance?
- Hydralazine
- Midodrine
- Alpha-1 agonists
- Beta Blockers
- Aspirin
Author of lecture Diuretics – Hypertension

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Prof. Alpert always manages to explain the subject in such a clear and simple way, it becomes easy to get and makes you remember everything in an orderly fashion.
