Playlist
Show Playlist
Hide Playlist
Cancer Drugs & Chemotherapeutic Agents: Dactinomycin, Doxorubicin, Bleomycin etc. – White Blood Cell Pathology

-
Slides Leukemia White Blood Cell Pathology.pdf
-
Download Lecture Overview
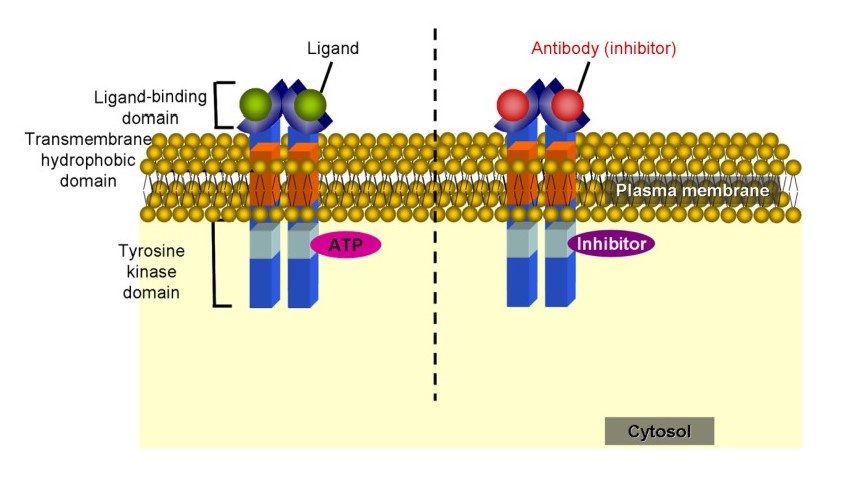
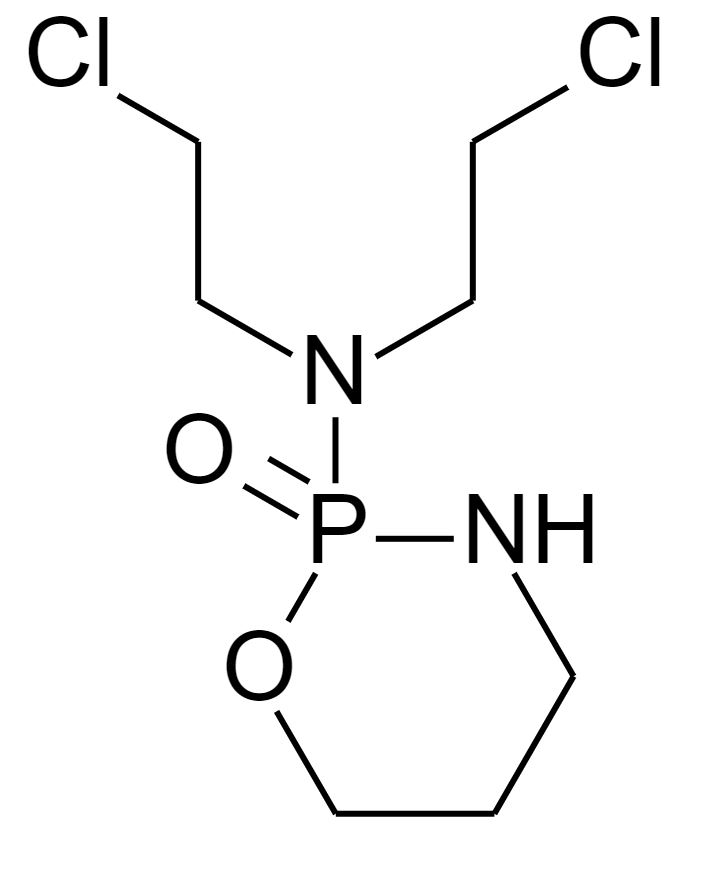
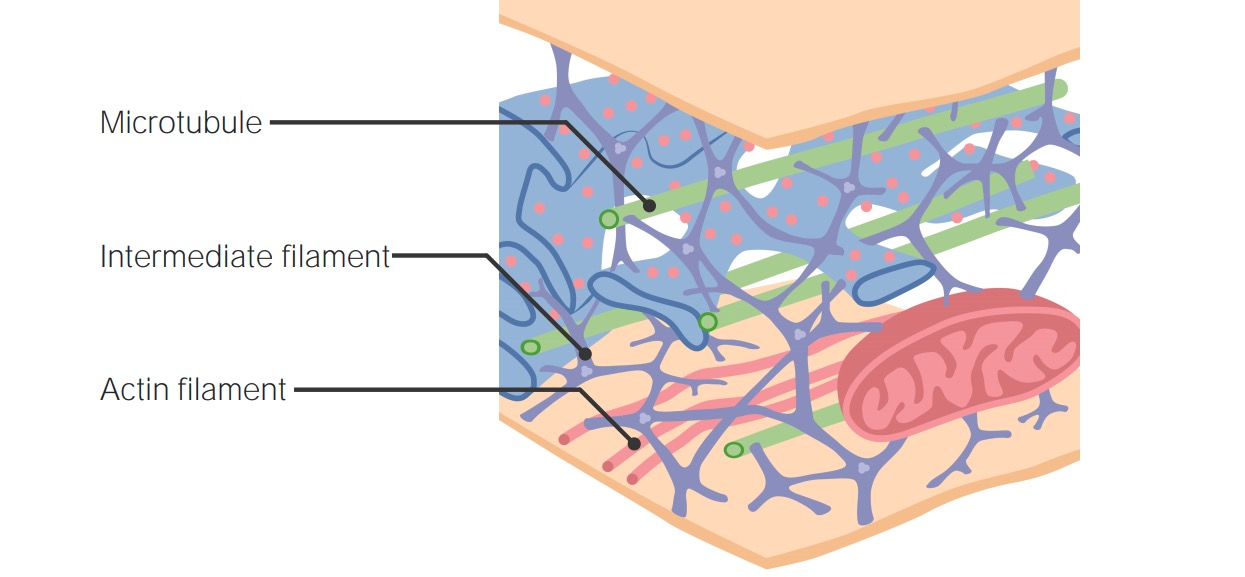
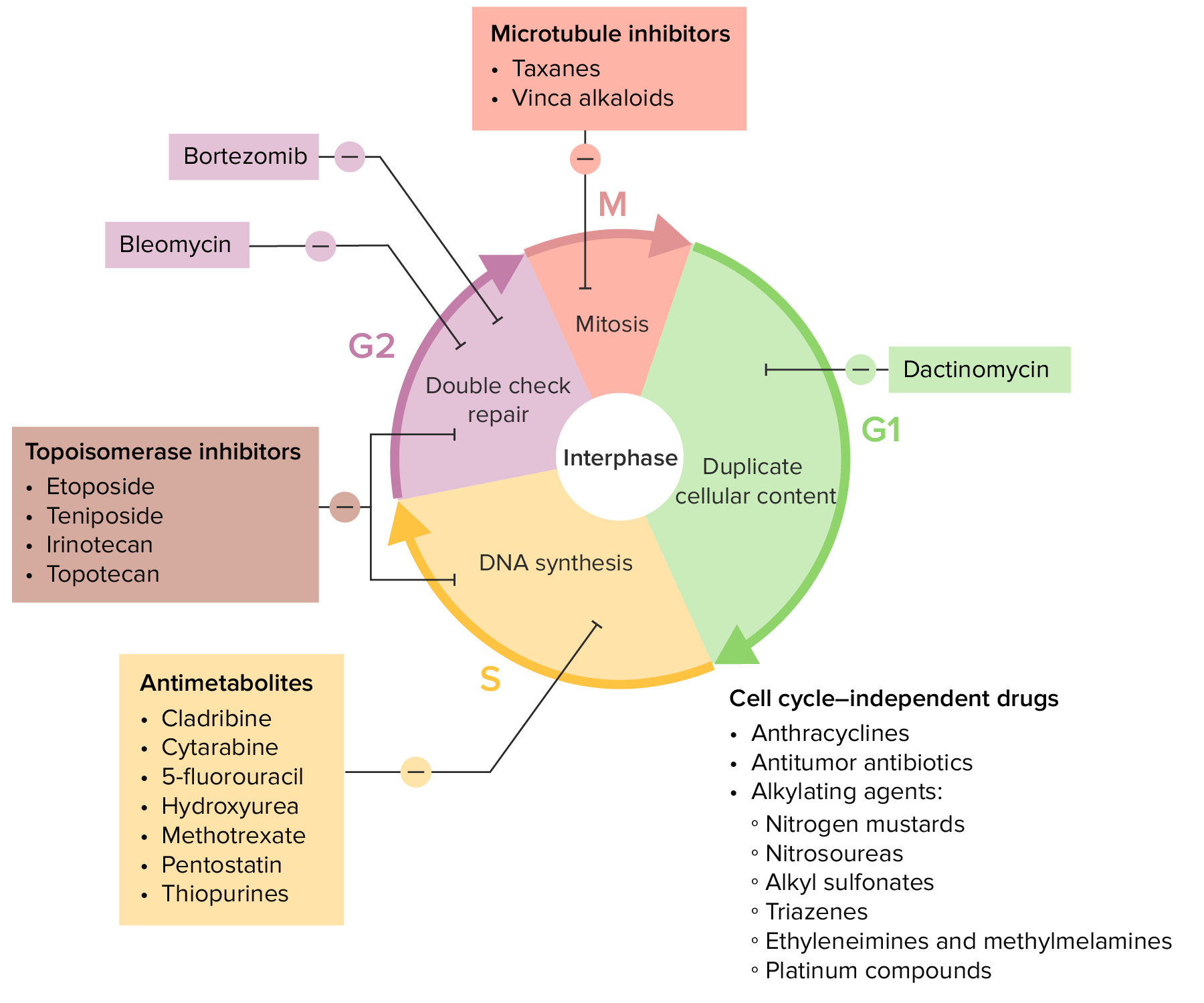
00:02 We have a drug here called dactinomycin. 00:04 You’d find that children might be acting out, so you’re looking at childhood cancers. 00:08 It intercalates the DNA, making it difficult for the DNA to properly carry its action. 00:14 So once you know it’s childhood cancers that you’re affecting, then you start thinking about the childhood cancers, Wilms tumor, the renal cell cancer in your child, Ewing’s sarcoma. 00:25 This is your translocation that you know about called 11;22, and you have involvement at the diaphysis of the bone in Ewing’s sarcoma. 00:34 Rhabdomyosarcoma, especially the young type, and you’re referring to embryonal rhabdomyosarcoma, a.k.a. sarcoma botryoides, usually used for childhood tumors. 00:47 Myelosuppressions, what are you looking for? Doxorubicin, Adriamycin. 00:51 Here, it generates free radicals, noncovalently intercalated DNA, breaks into DNA, and also inhibits replication. 01:01 So there are many points of your proper DNA mechanism or replication that completely slows it down. 01:07 The clinical uses: part of what’s known as ABVD, and this is your Adriamycin, which is part of regimen that you probably need to know for Hodgkin. 01:16 Also, used for myelomas, solid tumors, a lot of places. 01:21 In the process though, what you’re worried about definitely is cardiotoxicity, dilated cardiomyopathy, marked alopecia, and toxic tissue because of extravasation. 01:33 It actually comes out, cause damage to the tissue. 01:36 Doxorubicin, Adriamycin, ABVD, Hodgkin. 01:41 Bleomycin, a G2 phase inhibitor, specifically, includes a formation of free radicals. 01:48 Again, just like we saw with your doxy, and it breaks your DNA strand. 01:53 Can use this in testicular cancer. 01:55 It’s also part of your ABVD. 01:57 The B in ABVD is your bleomycin. 02:01 The A was Adriamycin, which is part of that doxorubicin. 02:04 Well, bleomycin, it may then cause pulmonary fibrosis, B and B, if that helps you. 02:10 Also, myelosuppression. 02:12 There, etoposide, or toposide, in general; teniposide and etoposide. 02:16 teniposide and etoposide. 02:18 Well, these are the drugs that then inhibit topoisomerase 2. 02:21 Therefore, it increases DNA degradation. 02:24 It’s used between S and G2. 02:27 It can be used for small cell lung cancer, which is also called oat cell. 02:31 If you want, take a look at the ETO in etoposide. 02:34 How would you pronounce OTE? Oh, ote, if that helps you. 02:39 So etoposide, oat cell cancer. 02:42 What’s another name for small cell? Oh, yes, oat cell cancer of the lung. 02:47 Also, testicular and prostate, and you’re worried about alopecia and myelosuppression, etoposide, topoisomerase 2, oat cell cancer of the lung, and testicular. 02:57 Cyclophosphamide, ifosfamide, covalently X-linked. 03:04 You need to memorize guanine N-7. 03:07 Bioactivation by the liver. 03:10 Non-Hodgkin’s lymphoma, hemorrhagic cystitis, look for blood in the urine, and maybe treated by giving mesna. 03:21 Know your couple of rescues, please. 03:23 Mesna, leucovorin. 03:26 Nitrosourea: You have carmustine, lomustine, semustine, lustines, requires bioactivation. 03:37 This, you need to make sure C –, carmustine, C – crosses the blood-brain barrier into the CNS. 03:45 Therefore, brain tumors, including GBM, glioblastoma multiforme. 03:52 Is it always effective? Unfortunately, it’s not. 03:55 May then, unfortunately, because of its crossing, cause CNS toxicity. 04:02 Busulfan: alkylates the DNA. 04:06 CML, also used for ablating bone marrow in hematopoeietic stem cell transplantation. 04:13 Don’t forget about that. 04:13 That’s big. 04:15 And here, once again, another B, busulfan, pulmonary fibrosis. 04:20 What was the other one that start with the B resulting in pulmonary fibrosis? Very good. 04:25 We had our bleomycin. 04:31 Here, we have our vinca alkaloids. 04:34 So, we’re in the M phase. 04:35 Vincristine and vinblastine. 04:38 Use the -cristine and the -blastine to advantage. 04:41 You’ll see why. 04:43 Mechanism, what does it do? Well, in the M-phase, it literally inhibits the polymerization of your microtubule. 04:50 And therefore, the microtubules will not properly pull your chromosomes apart. 04:56 That’s your vinca alkaloid. 04:58 It’s part of your MOPP regimen for Hodgkin, and this would then be oncovin, which is your vincristine. 05:06 Also, it could be used for choriocarcinoma, vincristine. 05:11 Toxicity. 05:12 Okay, the C in vincristine will be for CNS toxicity. 05:18 Also, oncovin, also choriocarcinoma, CCC. 05:24 If you’re dealing with vinblastine, it’s going to affect the bone marrow. 05:29 B – blastine, B – bone marrow suppression. 05:34 Vinca alkaloids. 05:37 Taxol, another method in which you can affect the M phase. 05:42 Here, literally, the spindle is not going to break down. 05:45 You’re going to inhibit taxing. 05:48 You can use this for, perhaps, ovarian and breast cancers in a female, obviously. 05:52 And hypersensitivity is what you’re looking for. 05:55 The paclitaxel and vinca alkaloids will be affecting your M phase. 06:00 Don’t forget though, the vinca alkaloids will behave by inhibiting the polymerization. 06:04 And then here, it will hyperstabilize the taxols, will hyperstabilize the polymerized microtubule. 06:11 In other words, it will freeze the “tubules” so that it doesn’t break down, therefore, cannot replicate. 06:20 Make sure that you know the actual medical pharmacologic language when dealing with vinca alkaloids, and also, taxols. 06:28 Hyperstabilization, inhibition of polymerization. 06:33 Cisplatin, carboplatin, plat-, your platinum drugs. 06:38 Cross-link DNA. 06:40 Testicular cancer, ovarian cancer. 06:44 Acoustic, acoustic nerve damage, eighth cranial nerve, platin. 06:51 Hydroxyurea: Last time you saw hydroxyurea was to then inhibit what’s known as -- or to help a patient increase your hemoglobin F. 07:02 It inhibits ribonucleotide reductase. 07:05 Memorize ribonucleotide reductase, hydroxyurea. 07:09 Next, it is used and could be used for melanoma, CML. 07:14 And the reason we have sickle disease, even though it’s not a cancer is the fact that it increases hemoglobin F. 07:21 In sickle cell disease, remember your completely deficient hemoglobin A, you’re then going to increase quite a bit of hemoglobin S when you have polymerization. 07:31 This is not good. 07:32 You are then going to or wish to increase hemoglobin F, which will then cause a left shift. 07:38 This is then going to also cause bone marrow suppression and GI upset. 07:44 Here, we have prednisone. 07:45 What is a steroid doing here? Well, it may trigger apoptosis, as we know. 07:50 Remember, the lymphopenia stuff that we talked about earlier. 07:54 It may even work on non-dividing cells. 07:56 Most common glucocorticoid in cancer therapy used in CLL, chronic lymphocytic leukemia. 08:02 May be part of that MOPP regimen, your last P. 08:06 We have also immunosuppressed. 08:08 Meaning to say that it may be used in autoimmune diseases, which then require immunosuppression. 08:13 Obviously, when utilizing prednisone, you’re worried about Cushing-like symptom, cataract, osteoporosis, everything that you would expect with prednisone or cortisol type of side effect, including your peptic ulcer disease in the stomach. 08:28 Here, we have our tamoxifen and raloxifene. 08:32 First and foremost, these are going to be your estrogen receptor modulators. 08:37 These are then going to behave as antagonist in the breast and agonist in the bone. 08:41 So therefore, these are partial agonists. 08:44 It will block the binding of estrogen to the estrogen receptor-positive cells. 08:49 You’re looking at your ER positive breast cancers. 08:53 Also, osteoporosis because it is going to be an agonist towards your bone. 08:58 We’re going to divide our tamoxifen, raloxifene as such. 09:01 Tamoxifen may increase the risk of endometrial cancer due to the partial agonist type of effective estrogen. 09:08 Whereas, raloxifene does not increase the risk of endometrial cancer because it is an endometrial antagonist. 09:16 Raloxifene seems to be a little bit better in terms of not having as much of a risk as tamoxifen. 09:23 Here, we have Herceptin or trastuzumab. 09:26 Your patient is HER-2/neu positive, which is Erb-B2. 09:29 HER-2 stands for human epidermal receptor growth factor. 09:34 This is a metastatic breast cancer or really, really Erb-B2 positive, extremely, extremely dangerous breast cancer, extremely cardiotoxic. 09:44 Imatinib would be used for 9 and 22. 09:48 We talked about tyrosine kinase. 09:50 It could also be used forth on a c-kit positive, or CD117. 09:55 And by c-kit, we mean that also, you’ve heard of gastrointestinal stromal tumor, and you could have tyrosine kinase there as well. 10:02 And so therefore, imatinib would be a drug to utilize in such issues. 10:06 CML and GIST, gastrointestinal stromal tumor, which is a smooth muscle benign tumor found in the stomach. 10:16 Rare, but of all the benign tumors in the stomach, GIST is the most common. 10:21 Fluid retention toxicity.
About the Lecture
The lecture Cancer Drugs & Chemotherapeutic Agents: Dactinomycin, Doxorubicin, Bleomycin etc. – White Blood Cell Pathology by Carlo Raj, MD is from the course Leukemia – White Blood Cell Pathology (WBC).
Included Quiz Questions
Which of the following drugs is cardiotoxic?
- Doxorubicin
- Bleomycin
- Etoposide
- Dactinomycin
- Cyclophosphamide
Which of the following cancer types is best treated with Imatinib?
- Chronic myelogenous leukemia
- Metastatic breast cancer
- Hodgkin’s lymphoma
- Melanoma
- Lung carcinoma
Which of the following drugs causes minimal myelosuppression?
- Bleomycin
- Etoposide
- Cyclophosphamide
- 5-fluorouracil
- Dactinomycin
What is the mechanism of action of Busulfan?
- Alkylates DNA
- Intercalate in DNA
- Inhibits reductase
- Inhibits topoisomerase II
- Free radical formation
What is the most commonly used glucocorticoid in cancer chemotherapy?
- Prednisone
- Beclomethasone
- Betamethasone
- Budesonide
- Cortisone
Author of lecture Cancer Drugs & Chemotherapeutic Agents: Dactinomycin, Doxorubicin, Bleomycin etc. – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
