Stevens-Johnson syndrome (SJS) is a rare, severe skin reaction, often caused by medications or infection.
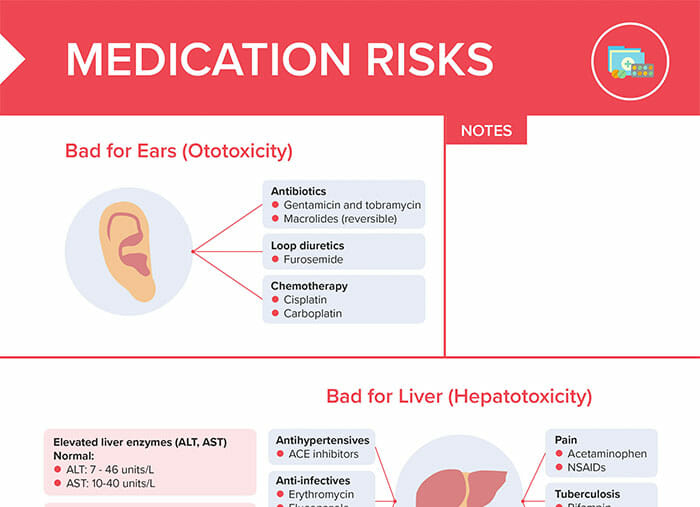
Common medication triggers include:
Genetic factors may also increase the risk of SJS reaction. Family members of clients with SJS should be counseled regarding their risk and the associated medications.
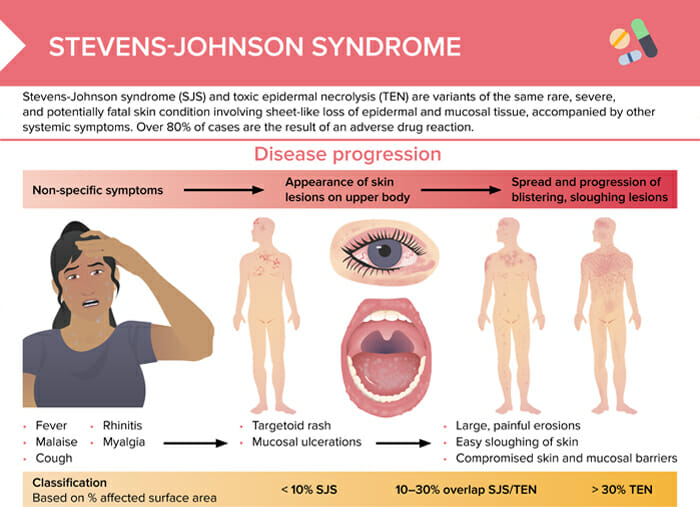
Toxic epidermal necrolysis (TEN) is the term for the most severe form of Stevens-Johnson syndrome.
Stevens-Johnson syndrome at first can present with non-specific symptoms like:
As the disease progresses, skin lesions appear (mostly on the upper body):
In the later stages, sloughing lesions and blistering spreads over the body:

Drug-induced toxic epidermal necrolysis with peeled skin over the back and buttocks.
Image: “Drug induced toxic epidermal necrolysis: two case reports” by Qadir SN, Raza N, Qadir F. License: CC BY 3.0Classification is based on the percentage of affected body surface area.
| Affected % | Classification |
| > 10 % | Stevens-Johnson syndrome |
| 10–30 % | Overlap SJS and TEN |
| > 30% | Toxic epidermal necrolysis |
The loss of a protective skin barrier may lead to extreme dehydration, infection, sepsis, shock.
Mucosal damage affecting the airway may lead to the client requiring mechanical ventilation. Damage to ocular tissue can cause blindness.
Acute organ dysfunction can affect pulmonary, cardiovascular, gastrointestinal, renal, and hematologic systems and may lead to multiple organ failure.
If a medication trigger is suspected, discontinue the medication as soon as possible.
Supportive care measures include:
High-dose systemic corticosteroid therapy may be considered.
Red man syndrome (RMS) and Stevens-Johnson syndrome (SJS) are both adverse reactions presenting with rashes, they are very distinct in terms of severity, risks, and treatment.
Red man syndrome is often due to rapid infusion of the antibiotic vancomycin. Slowing the infusion rate or pre-treatment with antihistamines are usually the only required treatment measures. Other than the relatively benign red man syndrome, Stevens-Johnson syndrome’s symptoms can progress to skin shedding and permanent damage, and can be life-threatening in its most severe form of epidermal necrolysis. Often, hospitalization in a burn unit or ICU is necessary.