T-tubes are catheters that drain bile into a bag outside of the body. They are placed in the common bile duct most often after complicated open cholecystectomies, and allow the bile duct to heal after the surgery. Find a summary below of the nursing tasks around T-tube care, and client education points.
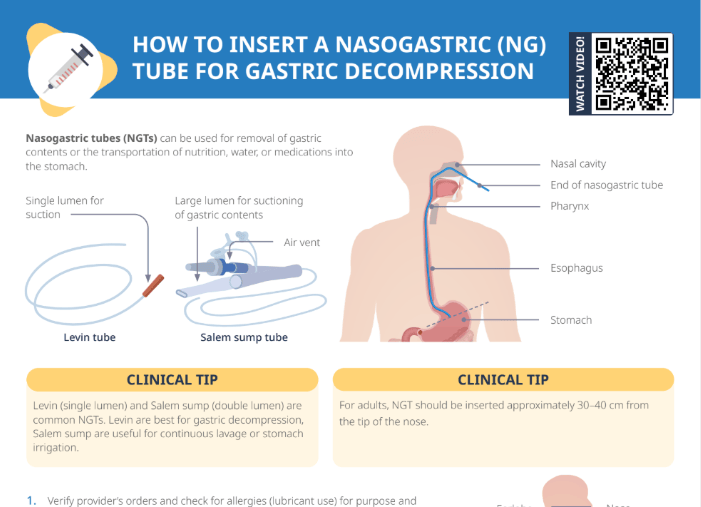
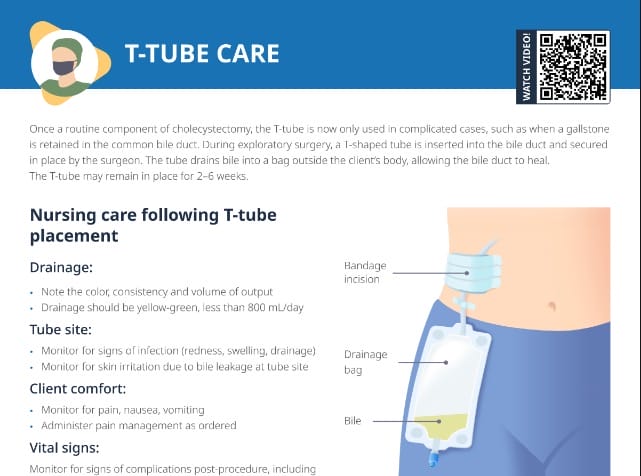
A T-tube is a transhepatic biliary catheter. It is a tube placed in the common bile duct that drains bile into a bag outside the body, allowing the bile duct time to heal.
T-tubes are most commonly placed after open cholecystectomies (removal of the gallbladder) and may remain in place for 2–6 weeks.
T-tube nursing care after open cholecystectomy
What is a cholecystectomy?
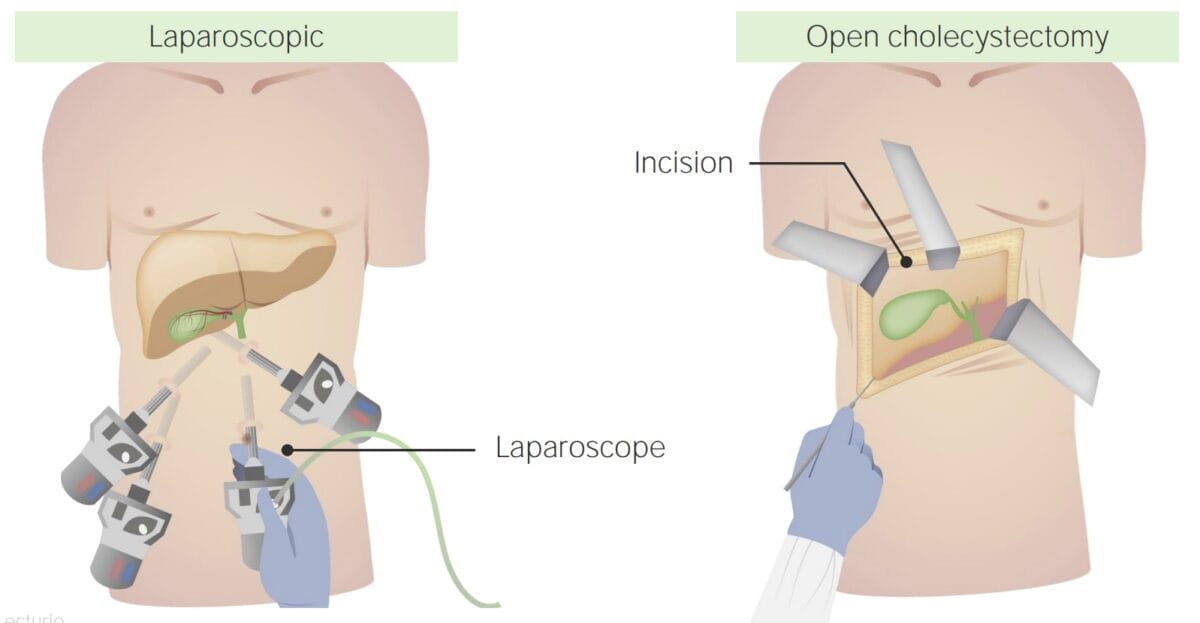
A cholecystectomy is a surgical procedure in which the gallbladder is removed. In an open or incisional cholecystectomy, it is removed through an incision in the abdominal wall. A T-tube may be placed in the common bile duct to keep the duct open while possible edema from manipulation during surgery resolves.
When and why are T-tubes placed after cholecystectomy?
While placing a T-tube used to be a routine component of cholecystectomies, it is now only used in complicated cases, such as when a gallstone is retained in the common bile duct. Due to the increasingly common laparoscopic cholecystectomy and improved surgical techniques, T-tubes are needed less frequently.
How much fluid does a T-tube drain after surgery?
Normally, the tube may drain up to 500 mL in the first 24 hours after surgery.
Drainage should decrease to less than 200 mL in 2–3 days and be minimal thereafter; with blood-tinged coloring initially changing to green-brown later on.
Nursing tasks around T-tubes after cholecystectomy
Priorities: Watch for signs of bleeding, bile leakage, T-tube obstruction, and infection. Monitor the client’s vital signs for signs of complications post-procedure, including fever and tachycardia.
Drainage:
Monitor the amount and color of the drained fluid.
Watch for signs of bile leakage or blocked/malfunctioning T-tube (e.g., sudden pain, nausea, fever, chills).
Tube site:
Monitor incision and watch for signs of infection (redness, swelling).
Cleanse the skin around the catheter site daily with an antiseptic.
Check for skin irritation due to bile leakage.
Change dressing daily:
Wash hands.
Remove old bandage.
Wash hands again.
Clean tube site with saline solution or mild soapy water.
Pat dry with clean gauze, put new bandage on the incision and tube site, and tape in place.
Make sure the bandage is large enough to cover the whole incision area.
Client comfort and education:
Manage the client’s pain.
Encourage activity.
Slowly introduce clear liquids and progress diet as ordered and appropriate.
Since clients may be sent home with T-tube still in place. Provide home-care instructions.
Patient education around T-tube care
General instructions when discharging a client with a T-tube
Clients should be encouraged to replace the amount of fluid drained into the T-tube bag with an electrolyte-rich liquid source.
Clients must be able to care for the T-tube following hospital discharge.
Instruct clients (how) to:
Avoid dislodging tube
Keep tube and insertion site clean and dry
Avoid kinks in tubing
Follow dietary restrictions as prescribed (low-fat diet)
Recognize and report signs of infection
Change the T-tube dressing every day or if it becomes wet or soiled
Further general education points:
Encourage practical steps toward a healthier lifestyle with smaller meals with lower fat.
Inform the client that they may experience yellow diarrhea for a few weeks from irritation due to bile salts until the body adjusts.
Encourage the client to talk about ways of increasing the activity level.
Reinforce medication education.
Drainage bag instructions
Note: For many patients, the T-tube is not connected to a drainage bag when they leave the hospital. They need to flush it 1–2 times a day with 10 mL of sterile saline, and should be instructed to clean the cap and the end of the tube with alcohol before flushing.
If a patient is sent home with a bag connected to the T-tube, further instructions are needed about how to empty the drainage bag:
Wash hands.
Remove the closure at the bottom of the bag.
Drain fluid into the provided measuring cup.
Record amount of fluid daily and report to the healthcare provider at the next visit.
Replace the closure on the bottom of the bag.
Wash hands again.
When to call the healthcare provider
Worsening pain
Nausea and vomiting
Fever or chills
Swelling or fluid leaking around the tube
New redness or warmth
More or new fluid draining from the incision
Incision not healing after 3–5 days
Stitches becoming sore, infected or loose
A bad smell from the incision site
Fluid that is light pink to dark red
A tube that stops draining or fell out
A yellow tint to the skin or increase itching
Note: Clients often have a hard time keeping long lists like this in mind. You can summarize the points to watch for into categories such as “Signs the tube is blocked and not working” and “Signs of infection” to make it easier for the client to keep an overview.
When is a T-tube removed?
The health care provider typically reviews an X-ray to ensure the duct has healed and there are no more stones before removing a T-tube.