What is done in a nursing skin assessment?
In a skin assessment, a full-body skin exam can be performed by nurses to examine the client’s skin systematically:
- Inspection: color, lesions, rashes, ulcers
- Palpation: temperature, moisture, turgor, edema/masses
- Assess:
- Wounds: size, surrounding skin, infection
- Hair, nails: texture, distribution, pests like lice, nail clubbing/ridges
What is skin turgor?
Skin turgor refers to the skin’s elasticity and how well it returns to its original shape. It gives insight into the state of the skin’s hydration. It can be assessed by pinching a fold of skin, as on the back of the hand, and then releasing it. If skin turgor is good, the skin quickly returns to its original position. If skin turgor is poor, the skin takes longer to reshape or remains elevated.
Skin assessment tools
Standardized tools or instruments can help guide skin assessment procedures, for example:
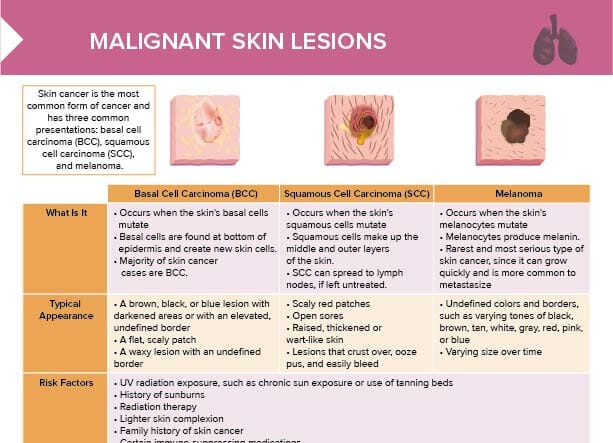
- ABCDE is a skin assessment tool and mnemonic used to evaluate skin lesions for skin cancer:
- Asymmetry (of moles/lesions)
- Border (irregular, ragged, blurred edges)
- Color (inconsistent)
- Diameter (larger than 6 mm, although melanomas can be smaller)
- Evolving (changes over time)
- Guided checklists
- Scoring systems for pressure injury stages
- Braden scale (predictive tool for pressure injury risk)
Skin assessment documentation
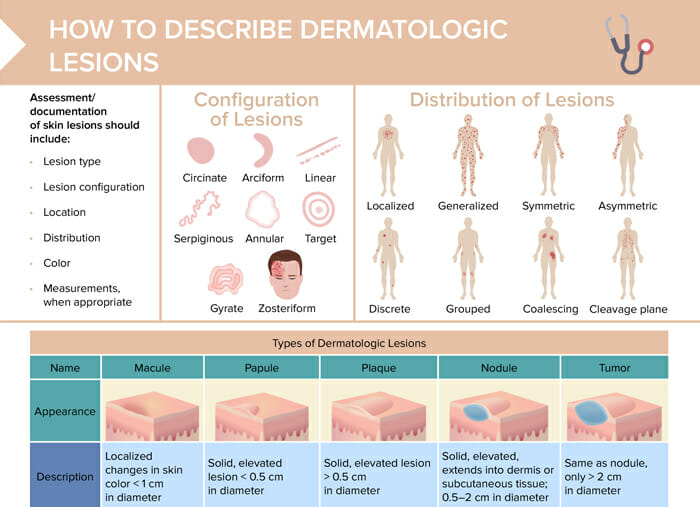
The documentation of skin lesions should include:
- Lesion type
- Lesion configuration
- Location
- Distribution
- Color
- Measurements
A skin assessment form may be used to facilitate documentation.
Using standardized terminology when describing skin lesions helps communication and efficiency in the healthcare team, and minimizes the risk of misinterpretations.
The configuration of lesions can be described as follows:
- Circinate
- Arciform
- Linear
- Serpiginous
- Annular
- Target
- Gyrate
- Zosteriform
The distribution of lesions can be categorized as follows:
- Localized
- Generalized
- Symmetric
- Asymmetric
- Discrete
- Grouped
- Coalescing
- Cleavage plane
Common skin lesions
- Macule: localized change in skin color, < 1 cm in diameter
- Papule: solid, elevated lesion, < 0.5 cm in diameter
- Plaque: solid, elevated lesion, > 0.5 cm in diameter
- Nodule: solid, elevated, extends into dermis or subcutaneous tissue, 0.5–2 cm in diameter
- Tumor: same as nodule, but > 2 cm in diameter
- Wheal: localized edema of epidermis causing irregular elevation
- Vesicle: elevated mass containing serous fluid, < 0.5 cm
- Bullae: same as vesicle, only > 0.5 cm
- Pustule: vesicle or bullae that become filled with pus
- Cyst: encapsulated fluid-filled or semi-solid mass
Nursing skin assessment examples
| Lesion | Examples |
| Macule | Freckle |
| Papule | Elevated nevi, seborrheic keratosis |
| Plaque | Psoriasis, eczema |
| Nodule | Lipoma, melanoma |
| Tumor | Breast carcinoma |
| Wheal | Insect bite, hive, angioedema |
| Vesicle | Herpes simplex, chicken pox |
| Bullae | Contact dermatitis, second-degree burns |
| Pustule | Acne, impetigo, furuncle, folliculitis |
| Cyst | Sebaceous cyst, epidermoid cyst |
Important skin assessment findings
The following are important skin assessment findings that are examples of findings that require monitoring for other conditions or diagnoses:
- Very pale skin may suggest anemia
- Cyanosis may suggest poor oxygenation
- Jaundice may suggest liver dysfunction
- Erythema can be from inflammation or infection
- Moles can indicate melanoma
- Rashes can be indicative of allergies
- Heat can be indicative of inflammation or infection
- Poor skin turgor can hint to dehydration
- Bruising can suggest clotting disorders or physical abuse