What makes giving medications to children challenging?
Research in pediatric populations is limited given the ethical considerations involved in conducting medical research on children.
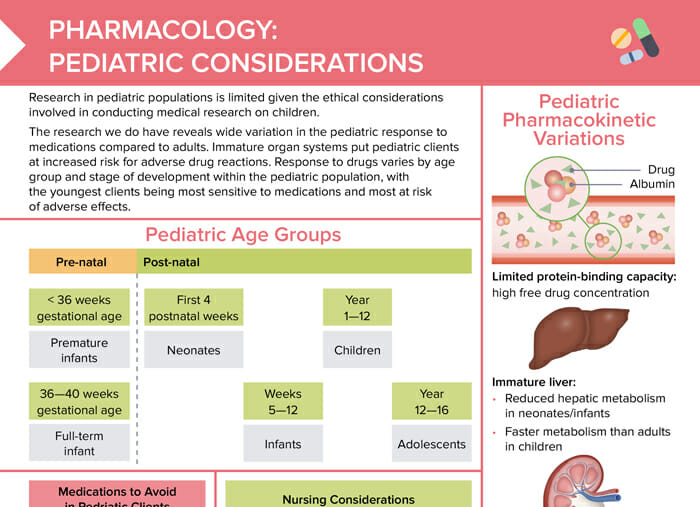
The research we do have reveals wide variation in the pediatric response to medications compared to adults. Immature organ systems put pediatric clients at increased risk for adverse drug reactions. Response to drugs varies by age group and stage of development within the pediatric population, with the youngest clients being most sensitive to medications and most at risk of adverse effects.
What are the pediatric age groups?
Prenatal
- < 36 weeks gestational age: premature infants
- 36–40 weeks gestational age: full-term infants
Postnatal
- First 4 weeks postnatal: neonates
- Weeks 5–12: infants
- Year 1–12: children
- Year 12–16: adolescents
Which medications should be avoided in children?
The following medications should be avoided in children:
- Aspirin (can cause Reye’s syndrome)
- Glucocorticoids (lead to growth suppression)
- Certain antibiotics:
- Chloramphenicol (risk of Gray syndrome in neonates and infants)
- Tetracyclines (can stain teeth)
- Fluoroquinolones (can cause tendon rupture)
Medication safety tips for nurses
- Pediatric drug doses are typically individualized based on weight.
- Calculate dosage carefully and validate calculations with a second nurse per facility protocol.
- Be aware of fluid volume balance and risk of volume overload when administering IV medications to pediatric clients.
- Be aware of choking hazards when administering oral medications to children.
- Build trust with clients and family.
- Educate family members on safe home medication administration.
Pediatric pharmacokinetic variations
Limited protein-binding capacity
Children’s bodies’ limited protein-binding capacity leads to a high free drug concentration.
Immature liver
Neonates and infants have a reduced hepatic metabolism; while children have a faster metabolism compared to adults.
Immature kidneys
Renal excretion is reduced in immature kidneys.
Underdeveloped blood–brain barrier
Pediatric clients’ blood–brain barrier not being fully developed leads to increased sensitivity to CNS medications.