Lung development involves 5 stages:
Tip: Remember those stages with “Every Pulmonologist Can See Alveoli!”
In the embryonic stage, the trachea and the primary bronchial buds develop.
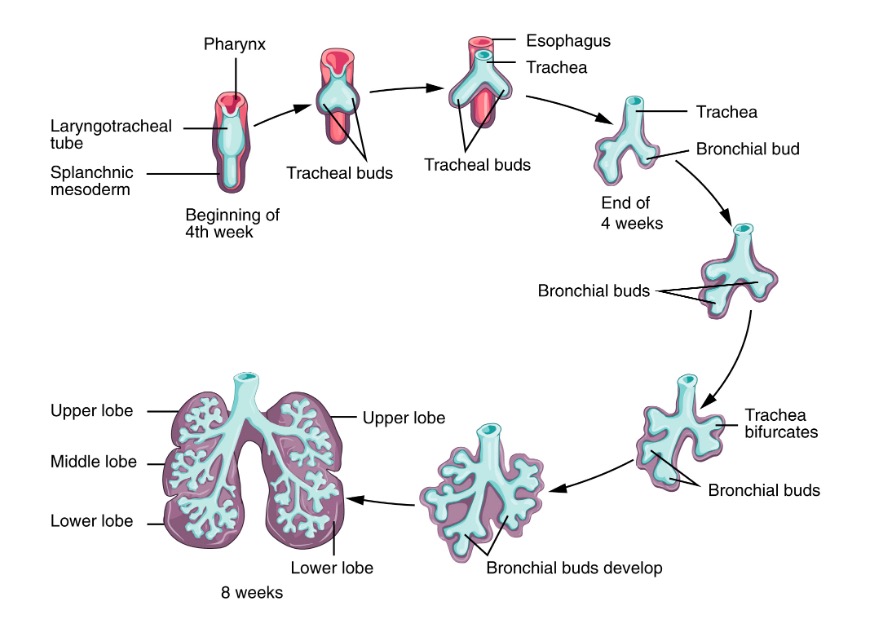
Early stage of lung development:
During the early stages of lung development (embryonic and pseudoglandular), the lung bud gradually transforms into the trachea and then bifurcates, forming the two mainstem bronchi. These bronchi will further divide, giving rise to lobar and segmental bronchi.
Main steps of the pseudoglandular stage involve the development of the bronchial tree.
Note: The first breathing movement can be detected around 10 weeks of gestation, however, since the respiratory bronchioles don’t develop until the next stage, the fetus cannot survive at this point yet.
In this stage, the respiratory units (canaliculi) develop. By the end of the canalicular stage, the fetus is capable of enough respiration to survive with intensive care.
In the saccular stage, the alveoli begin to mature, capillary networks grow, and surfactant production increases significantly.
The respiratory units grow and mature further throughout this time: goes from 50 million alveoli at birth to 300 million by age 8 (with rapid increase in the first 6 months).
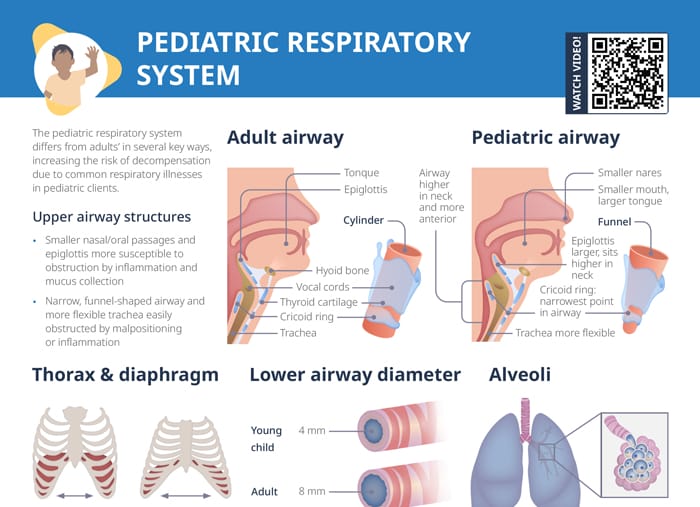
Tip: As we know, children are not just “small adults.” Their physiology and anatomy varies in significant ways that require specialized treatment and open up the possibility for different conditions than adults are affected by.
In children, the diaphragm fatigues more easily. The accessory muscles are immature and weaker, and the increased rib cage angle and relatively large organ size limit chest expansion. Increasing the respiratory rate is the only mechanism to increase lung function in children.
At birth, children have a much smaller number of functioning alveoli, so the area for gas exchange is much smaller. The small, immature alveoli are more susceptible to collapse and atelectasis.
Lung surfactant is a phospholipid produced within the alveoli that reduces surface tension and keeps the alveoli open. It is produced at 30–34 weeks gestation and will be insufficient in premature infants.
Insufficient surfactant may cause:
Tone should be flat over bony structures, organs, and muscles, resonant over lung tissue.
Inspection:
Palpation:
Percussion:
Dull sound over lung fields can indicate pneumonia or other lung infiltrations.
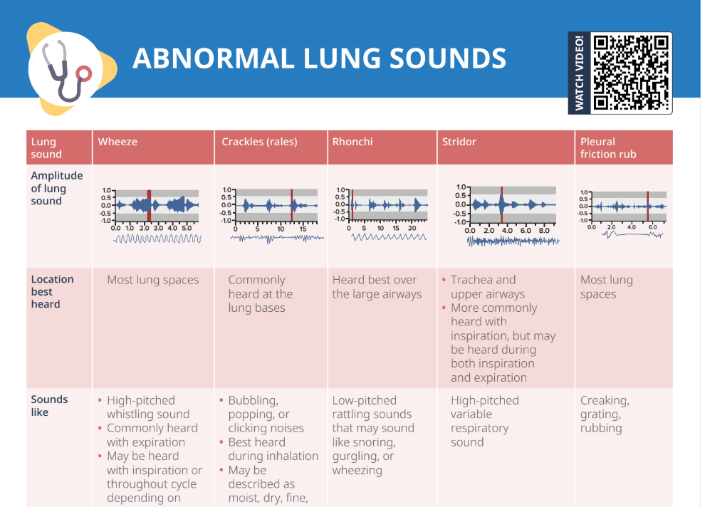
Auscultation: