Lithium, a mood stabilizer, has been a cornerstone in the treatment of bipolar disorder and some forms of depression for decades. In clinical nursing practice, lithium requires close monitoring due to its narrow therapeutic window and severe potential adverse effects of toxic doses. Keep reading for nursing considerations around lithium treatment and the most important patient education points.
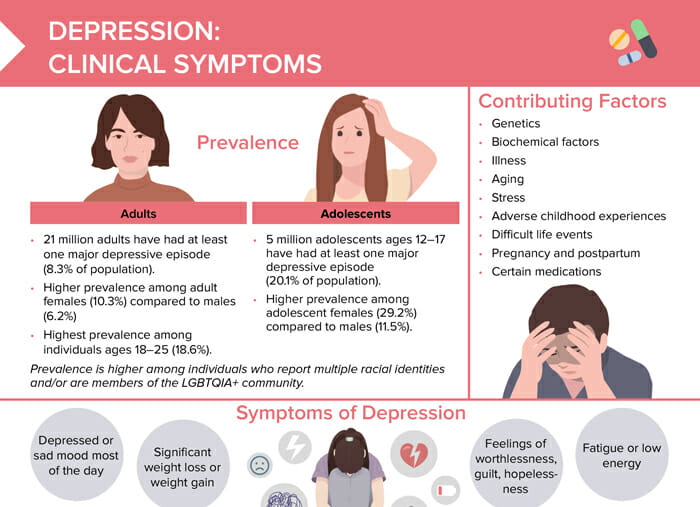
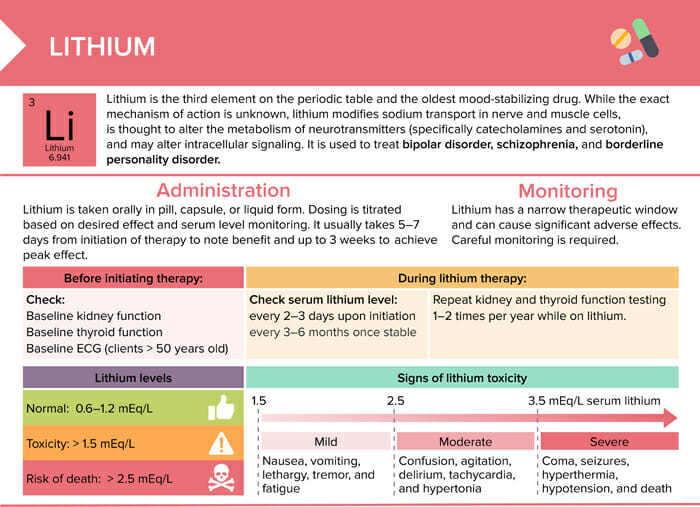
Lithium is the third element on the periodic table and the oldest mood-stabilizing drug. It is used to treat bipolar disorder, schizophrenia, and borderline personality disorder.
Lithium methods of administration
Lithium is taken orally in pill, capsule, or liquid form. Dosing is titrated based on desired effect and serum level monitoring. It usually takes 5–7 days from initiation of therapy to note benefit and up to 3 weeks to achieve peak effect.
While the exact mechanism of action is unknown, lithium modifies sodium transport in nerve and muscle cells, is thought to alter the metabolism of neurotransmitters (specifically catecholamines and serotonin), and may alter intracellular signaling.
Lithium: nursing considerations and interventions
Lithium has a narrow therapeutic window and can cause significant adverse effects. Careful monitoring is required.
Before initiating lithium therapy
Check baseline kidney function
Check baseline thyroid function
Baseline ECG (clients > 50 years old)
During lithium therapy
Check serum lithium level every 2–3 days upon initiation and every 3–6 months once stable
Repeat kidney and thyroid function testing 1–2 times per year
Common early side effects of lithium
Gl distress (nausea, bloating, diarrhea)
Fatigue
Muscle weakness
Headache
Confusion
Memory impairment
Polyuria and thirst
Client education points about lithium
Help clients know what to expect in terms of side effects. Early symptoms often resolve with time. Report if severe/persistent.
Teach clients to maintain normal dietary sodium intake.*
Teach clients to increase their fluid intake. Lithium blocks the effects of ADH, causing increased urine output (can lead to hypovolemia).
Diarrhea can lead to sodium loss, putting clients at risk of lithium toxicity. Clients should be alert to signs of toxicity and notify their provider of diarrheal illness.
Educate clients to consult their provider before taking drugs that affect lithium levels, including:
Diuretics
NSAIDs
Antihistamines
ACE inhibitors
Metronidazole
*Lithium is a positively-charged ion and is processed like sodium by the kidneys. Low serum Na+ causes the kidneys to retain Li+ along with sodium. Li+ retention can lead to toxicity.