Discharge planning has the goal of making a client’s transition from the hospital to the next level of care safely and smoothly. The process already starts when a client is admitted and involves assessing client care needs, client education, addressing barriers to discharge, and coordination of follow-up and services.
Last updated: January 20, 2026
RELATED STUDY SHEET
Overview of common discharge instructions including referrals and when to notify for complications.
Discharge planning is the process of preparing clients for the transition from the hospital to the next level of care. Clients may be discharged to home, a rehabilitation facility, or other settings.
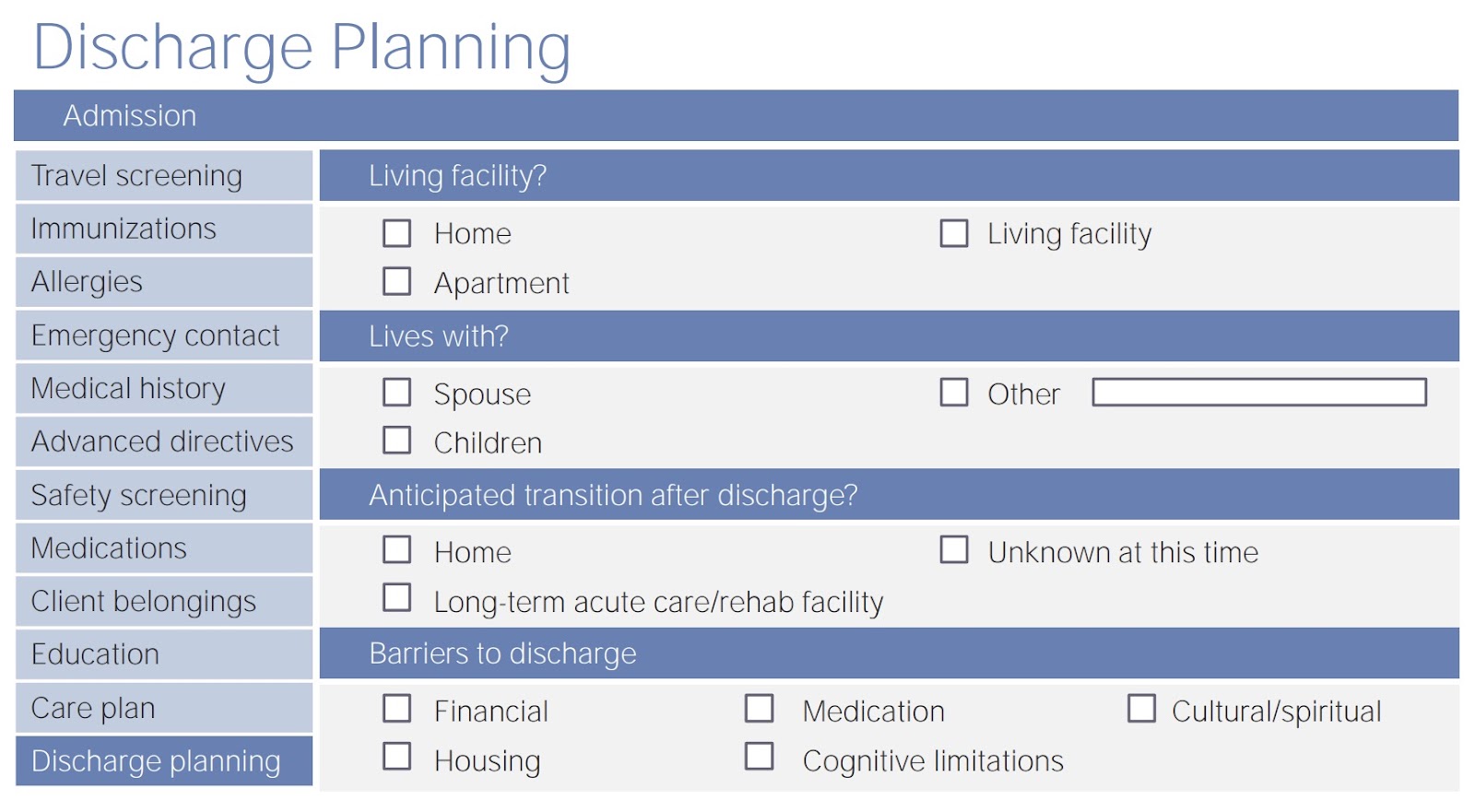
Nursing tasks around discharge planning include:
Assessing the client’s readiness for discharge
Client and family education about care needs
Coordination with other healthcare professionals about ongoing care, appointments, and equipment
Identify and manage barriers to discharge
Developing a reliable, effective discharge plan helps to prevent readmissions and improves client satisfaction and outcomes.
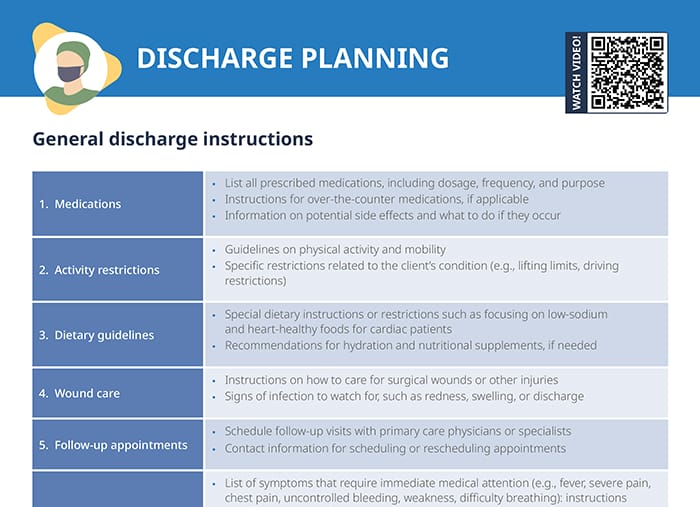
List all prescribed medications, including dosage, frequency, purpose, and time of last dosage given
Instructions for over-the-counter medications, if applicable
Information on potential side effects and what to do if they occur
Activity restrictions
Guidelines on physical activity and mobility
Specific restrictions related to the client’s condition (e.g., lifting limits, driving restrictions)
Dietary guidelines
Special dietary instructions or restrictions, such as focusing on low-sodium and heart-healthy foods for cardiac clients
Recommendations for hydration and nutritional supplements, if needed
Wound care
Instructions on how to care for surgical wounds or other injuries
Signs of infection to watch for, such as redness, swelling, or discharge
Follow-up appointments
Schedule follow-up visits with primary care physicians or specialists
Contact information for scheduling or rescheduling appointments
Symptoms to monitor
List of symptoms that require immediate medical attention (e.g., fever, severe pain, chest pain, uncontrolled bleeding, weakness, difficulty breathing): instructions to call 911 or go to the nearest emergency room
List of symptoms that should be reported to the healthcare provider within 24–48 hours, such as fever over 101ᐤ, increasing pain, persistent vomiting, or changes in mental status
Specific signs of complications related to the client’s condition
Referrals and case management
Referrals to specialists
Detailed instructions on appointments with referred specialists
Contact information and reasons for referral
Home health services
Information on any arranged home health care, including nursing visits or physical therapy
Contact information for home health providers
Case manager involvement
Name and contact information of the case manager assigned to the client
Description of the case manager’s role in coordinating care and follow-up
Nursing discharge examples
Discharge plan example
Client: John Doe
Diagnosis: Heart failure
Discharge date: July 20, 2024
Medications:
Furosemide 20 mg once daily in the morning.
Metoprolol 50 mg twice daily.
Lisinopril 10 mg once daily.
Aspirin 81 mg once daily.
Potassium supplement as needed.
Diet and activity:
Follow a low-sodium diet; avoid salty foods and read food labels carefully.
Fluid restriction: Limit to 1.5 liters per day.
Engage in light physical activities such as walking for 20-30 minutes daily, gradually increasing as tolerated.
Avoid strenuous activities until cleared by the cardiologist.
Follow-up appointments:
Cardiologist: Dr. Smith on July 27, 2024, at 10:00 AM.
Primary care physician: Dr. Johnson on August 3, 2024, at 9:00 AM.
Self-monitoring and symptoms:
Monitor weight daily and record it; report a weight gain of more than 2 pounds in 24 hours or 5 pounds in a week.
Watch for symptoms of worsening heart failure: increased shortness of breath, swelling in legs or ankles, fatigue, or coughing.
Call the healthcare provider if symptoms worsen or if there are any new symptoms.
Education:
Reviewed signs and symptoms of heart failure exacerbation.
Provided educational materials on heart failure management and lifestyle modifications.
Discussed the importance of medication adherence and follow-up visits.
Home health services:
Home health nurse visits twice weekly for the next month to monitor weight, vital signs, and medication adherence.
Physical therapy evaluation to develop a safe exercise program.
Nursing discharge note example
Date: July 20, 2024
Time: 11:00 AM
Client: John Doe
Room: 203
Nurse: Jane Smith, RN
John Doe, a 65-year-old male, is being discharged today following treatment for heart failure. The client is alert, oriented, and has been educated on the discharge plan. Vital signs are stable: BP 120/80, HR 75, RR 16, SpO2 98% on room air.
The client has been provided with prescriptions for furosemide, metoprolol, lisinopril, and aspirin, as well as instructions on potassium supplementation. Detailed instructions on a low-sodium diet and fluid restriction have been given, and the client demonstrated understanding by verbalizing the key points. Activity recommendations have been discussed, emphasizing the importance of gradual increases in physical activity.
Follow-up appointments with Dr. Smith (cardiologist) and Dr. Johnson (primary care physician) have been scheduled, and the client has been advised on the importance of attending these appointments. The client was instructed to monitor daily weight and report any significant weight gain or symptoms of heart failure exacerbation.
Educational materials on heart failure management were reviewed with the client, who confirmed understanding. Arrangements for home health services, including nursing visits and physical therapy, have been made to support the client post-discharge.
The client and spouse expressed understanding of the discharge plan and were given contact information for the healthcare team in case of questions or concerns. All questions were addressed, and the client stated “I will follow these instructions” with the discharge instructions in hand.
Frequently asked questions
Can a nursing home discharge a client with nowhere to go?
Nursing homes are generally required to follow specific regulations and guidelines when discharging a client, ensuring that the discharge is safe and that the client has a suitable place to go.
What is voluntary discharge from a nursing home?
A voluntary discharge from a nursing home occurs when a /client/resident decides to leave the facility on their own accord, rather than being discharged by the facility.
What is unsafe discharge from a skilled nursing facility?
An unsafe discharge from a skilled nursing facility refers to the process of releasing a client without adequate planning or ensuring their safety and well-being post-discharge with proper support.