What is allergic rhinitis?
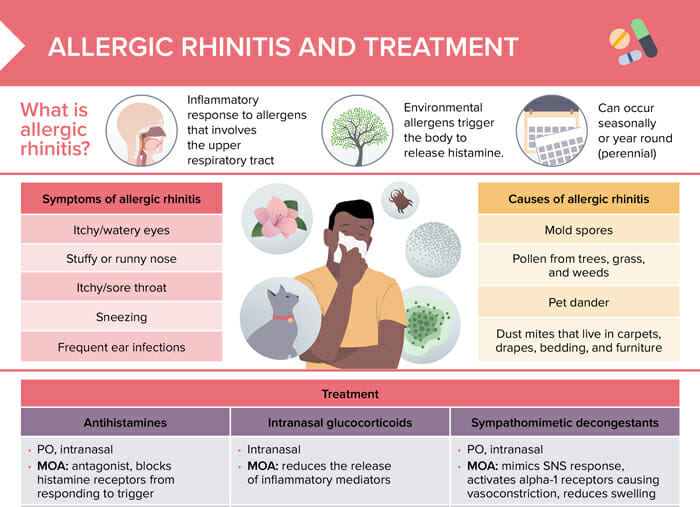
Allergic rhinitis is an inflammatory response to environmental allergens that involves the upper respiratory tract. It is often referred to as hay fever and can be seasonal or perennial.
What causes allergic rhinitis?
Common environmental allergens that can trigger allergic rhinitis include mold spores, pet dander, pollen from trees, grass, and weeds, and dust mites that live in carpets, drapes, bedding, and furniture.
What are the symptoms of allergic rhinitis?
Symptoms of allergic rhinitis include itchy/watery eyes, itchy/sore throat, frequent ear infections, stuffy or runny nose, and sneezing.
How to treat allergic rhinitis
Treatment options for allergic rhinitis include antihistamines, intranasal glucocorticoids, sympathomimetic decongestants, immunotherapy, and saline nasal irrigation.
Antihistamines
- PO, intranasal
- Method of action (MOA): antagonist, blocks histamine receptors from responding to trigger
- 1st generation: diphenhydramine (causes sedation)
- 2nd generation: fexofenadine, loratadine, cetirizine (non-sedating)
- Intranasal: azelastine
Intranasal glucocorticoids
- Intranasal
- MOA: reduces the release of inflammatory mediators
- 1st generation: beclomethasone, budesonide, triamcinolone (more systemic effects)
- 2nd generation: ciclesonide, fluticasone propionate (less system effects)
- More effective than antihistamines
Sympathomimetic decongestants
- PO, intranasal
- MOA: mimics SNS response, activates alpha-1 receptors causing vasoconstriction, reduces swelling
- Phenylephrine, pseudoephedrine
- Contraindicated in clients with HTN, cardiovascular disease d/t vasoconstriction
- Requires ID to purchase d/t use in crystal methamphetamine production
How to educate clients about allergic rhinitis
- Clients should be educated on how to reduce exposure to triggers; however, prevention is not always possible.
- Immunotherapy is a long-term treatment option for clients with moderate to severe allergic rhinitis.
- Saline nasal irrigation may reduce symptom severity.
- Avoid using intranasal sprays for more than a few days (potential for abuse). Wean to avoid rebound congestion.