Interleaving is (Desirably) Difficult
In a previous article, we discussed the importance of understanding the different types of memory and acknowledged their critical role in medical education. Both teachers and learners need to be familiar with the concepts of declarative and procedural memory, as well as how these memory systems work, in order to maximize knowledge retention and boost student performance. The aim of utilizing both systems is ultimately to build elaborate mental schemas that students can refer to when applying learned concepts and use as scaffolds to facilitate the acquisition of new knowledge and skills. Schemas interlace neural links from the procedural and declarative systems that build on preexisting knowledge to form more elaborate neural connections and facilitate deeper understanding.(1)
Although we will explore schemas in depth in another article, a key message is that the strength of these schemas (and in turn the extent to which they facilitate learning) relies on strategies that employ what Robert Bjork calls desirable difficulties.(2) To illustrate, consider how the symptoms of anemia can be taught. One way would be to present the symptoms and ask the students to read them. This task is simple and requires minimal cognitive effort, but the information would naturally dissipate and be forgotten, probably within a few minutes.
However, if the teacher starts off by asking the students what they think the symptoms of anemia are, they will utilize more cognitive effort while trying to come up with the symptoms. The information is thus more likely to be retained and for a longer period. Put simply, adding difficulty has a positive impact on learning—up to a certain point, that is. Desirable difficulty is based on the notion that the more effort required to retrieve something, the better it is learned(3), unless the task is too difficult—if the learner lacks some essential background knowledge or skill, for example.(4)
In the following sections, we take a deeper look into one of the common learning strategies that make use of desirable difficulties: interleaving. We will explore the evidence behind the strategy, explain how and why it works, and provide recommendations for enhancing medical education, for teachers and for learners.
What is Interleaving?
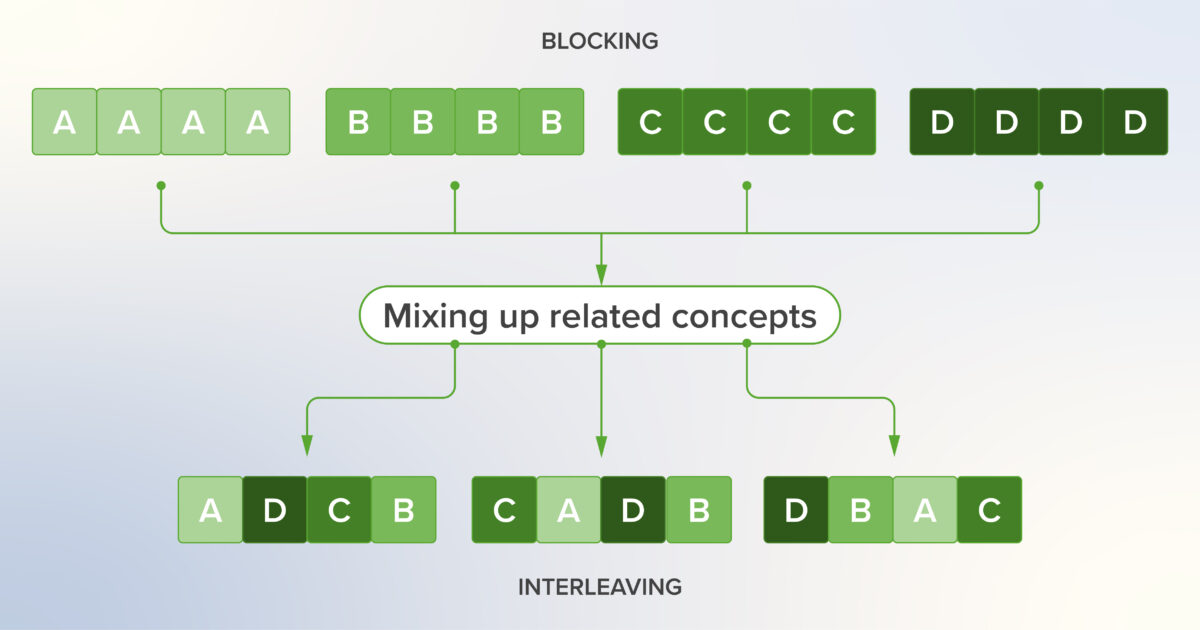
Interleaving is the practice of varying or mixing up related concepts being taught/learned, as opposed to studying them in a blocked fashion. Interleaving results in the creation of stronger and better neural connections by engaging the students’ neocortex to recognize subtle differences between divergent but overlapping sets of neural links.(1) Interleaving may assist with transfer(5)—the ability to apply learning to other situations—which is precisely the goal of a medical practitioner.
A simple example from mathematics for students learning to perform arithmetic operations with fractions is illustrated below.
Instead of practicing multiplication followed by other operations (blocked practice), the exercises are mixed up (interleaved practice)

The problem with blocked practice is that it is less beneficial with respect to the time investment it requires, although it is perceived as faster and easier by students.(6) In blocked practice, students learn how to solve a given problem and then go on to solve multiple similar problems with little added benefit (example above). Yet, this is preferred by students because it creates an illusion of knowing—because they are “looping information through short-term memory without having to reconstruct the learning from long-term memory”.(3)
Owing to its perceived difficulty, interleaving seems like a counterintuitive strategy. Indeed, students usually avoid this study technique because they do not feel like they are making as much progress as when using blocked practice, but this perception is erroneous. The desirable difficulty this strategy brings about adds an element that is usually underutilized in education: the importance of teaching students not only how to tackle a problem but also when to use the knowledge and skills they have learned to tackle a problem.(1) For example, when students are given a set of cases to solve that are mixed up, they cannot anticipate how to approach those problems the same way as when they are given a set of cases within a particular discipline.
It is crucial to note, however, that for the interleaved strategy to work, the exercises/concepts need to be similar and related to a certain extent. Interleaving cardiac electrophysiology with glycolysis, for example, is not going to yield any benefit.(7) This is because the value of interleaving lies in the fact that students learn to differentiate between concepts that have subtle differences. This also forces students to maximize the use of their procedural memory (an essential tool for health care professionals) as they learn to detect and differentiate patterns by applying their knowledge.(8)
To illustrate, we can look at the following concepts from medicine: anemia, hypoglycemia, hypothyroidism, and depression (figure below). Students in an advanced stage of their training have already covered these pathologies and would know that they can have similar clinical presentations. When students learn and practice cases with these concepts separately, they are taking a blocked approach and developing individual schemas for those concepts. They can master these topics and do well on a quiz that tests these concepts separately. In a real patient encounter (or in a final cumulative examination), however, they will have to distinguish between those conditions that have similar presentations in order to manage a patient presenting with fatigue appropriately. Interleaved practice thus allows students to learn and practice these topics together, developing links between their separate schemas and preparing them for actual scenarios that they might encounter in their careers. In fact, creating a differential diagnosis is an exercise in interleaved practice.
Medical example of interleaving visualizing relationships between neocortex and working memory

Further to the above, this example illustrates how interleaving can be tricky to implement—if these four concepts were interleaved and presented to students in an early stage of their training who were not yet familiar with them, it would be too (undesirably) difficult to make connections, leaving the students confused and frustrated.
Interleaving is applied extensively and effectively in sports training.(9) Rather than practicing specific maneuvers repeatedly before moving on to the next one (passing the ball vs shooting the ball in basketball), players are encouraged to mix up their practice, and their training routines are in fact designed to facilitate that approach. This works very well owing to the extent of involvement of the procedural memory system in sports. The practice of medicine also relies heavily on procedural memory, and the training routines of doctors should also benefit from an interleaved approach.
Interleaving: Insights From the Classroom
Interleaving as a learning strategy was initially assumed to be less effective compared with blocked practice. This hypothesis was tested on students by Kornell and Bjork in 2008.(10) In that study, art students were better able to determine differences between painter styles when they initially learned them in an interleaved manner, thus contributing convincing evidence contrary to the prevailing assumption and demonstrating that interleaving is superior to blocked practice. That study also indicated that students’ metacognitive ability is limited; they thought they learned better with blocked practice.(10) Future studies would go on to show that the same benefit of interleaving is seen with learning science concepts.(8,11,12)
The research suggests that there are two possible mechanisms by which interleaving enhances learning:
- Attention attenuation: Repeated examples that are similar will result in faded attention of students and a mechanical rather than cognitive approach.
- Discriminative contrast: Interleaving grants more opportunities to compare and contrast different concepts.
There is evidence in the literature to demonstrate the effectiveness of interleaving in medical education as well.(12) Studies have shown that interleaving provides an advantage for knowledge transfer to more complex problems,(7,13,14) highlighting its potential for improving diagnostic problem-solving.(15) For example, a 2003 study by Hatala et al. examined the role of mixed practice for the acquisition of ECG interpretation skills. In the study, students were split into two groups: one that practiced ECG interpretation in a blocked manner and one that employed interleaved learning (figure below). Not surprisingly, the experiment showed that the students who took an interleaved approach performed better in terms of diagnostic accuracy than those who practiced in blocks (46% vs 30% accuracy).(11)
Medical education example of utilizing interleaving vs blocked practice with ECG interpretation(11)

A study on psychology students also demonstrated that those who mix their practice are more likely to do better on examinations that involve knowledge transfer and the application of learned concepts to new contexts.(16)
Implementation of Interleaving in Medical Education
Implementing interleaving might not be straightforward, especially in medical education, owing to challenges in implementation within traditional educational settings and the long-established practice of the traditional blocking of medical topics.
There are several things to consider in order to implement interleaving:
- Who will be responsible for implementing this study technique? Students, teachers, administrators?
- What subjects/concepts can be interleaved? How similar or different should they be?
- What specific examples exist in medical education and how have they been implemented?
- Has an adequate knowledge foundation been established to allow for effective interleaving (comparing and contrasting concepts)—it is difficult to compare and contrast concepts which one does not understand in the first place!
Interleaving is essentially mixing up practice of related elements. This is simple to do in the clinical years of medical school and occurs naturally in a clinical environment—each patient experience offers a different set of exercises and concepts, most of which are related. With repeated exposure over time, students become more familiar with the nuances between medical topics and begin to master and apply them in practice. In the preclinical environment, it is less natural. Educators tend to teach things in blocks and students are tested in blocks, so they also study in blocks. A curricular approach that incorporates a case-based format from the early stages of the educational process attempts to apply interleaving in the basic science curriculum but depends on having students with a good knowledge foundation and who are particularly adept at drawing associations.
A possible, yet challenging way to implement interleaving in medicine is through the spiral curriculum approach, a curriculum model based on cognitive theory advanced by Jerome Bruner. In this approach, the same topic is introduced to learners at different stages of their studies, increasing in depth and complexity.(17) When applied properly and with an accurate understanding of the learners’ comprehension levels, this design can allow learners to benefit from interleaving. However, incorrectly applied (e.g., owing to insufficient points of relatedness or lack of distinguishing features between topics), a barrier to understanding and a negligible beneficial impact may result. It is thus important to take ample care when utilizing this curricular model as your means of incorporating interleaving into daily learning; when in doubt, start with smaller blocks of topics over smaller periods of time.
Simulations are a prototypical example of interleaving in education. Simulations mimic real-life scenarios with patients, requiring students to demonstrate their medical knowledge, bedside manner, physical examination skills, and laboratory and imaging interpretation skills. Ultimately, the interleaving practiced in medical simulations increases practitioners’ diagnostic accuracy as well as their ability to develop patient management plans. Students who practice in an interleaved fashion, rather than blocking between medical knowledge, physical examination skills, etc., ultimately perform better in clinical work.(3)
With these examples in mind, proper implementation of interleaving thus needs a two-pronged approach: (a) implementing changes in the medical curricula and (b) encouraging students to follow these strategies when they study.
Educator’s perspective:
- Educators should mix up their practice by going back and forth between similar topics. For example, in teaching the subjects of coronary artery histology and acute coronary syndrome, using learning objectives as a guiding point to decide which topics are related, which are not, and which can be compared and contrasted to each other is very helpful, underlining once again how learning objectives can act as a springboard from which many effective learning techniques can be adapted, combined, or optimized.
- Educators can teach different but related pathologies in the same class. For example, teaching differential diagnoses of anemia, followed by a session on haematological cancers, could help students draw parallels between the different types of anaemia and certain aspects of haematological cancers (pathophysiology, effect on CBC readings, symptoms) and encourage them to identify differences between these two conditions (underlying mechanism, severity of symptoms, survival rate, etc.).
- Educators could use a case study approach by asking students to interpret laboratory results and discuss other presentations that could explain these results. For example, an atypical CT scan with brain edema could be due to diabetic ketoacidosis, an intracranial bleed secondary to trauma, a tumor, etc. These different conditions can be explained thoroughly or can be discussed interactively within a group.
Key application tips to keep in mind:
- Educators could use interleaving in combination with spacing by filling spaced out concepts with highly related ones. This way, the materials are both spaced over time and varied.(18)
- While interleaving emphasizes the importance of varied practice, there is a risk of underemphasizing repeated retrieval practice on the basics—it is not variety vs repetition. Combining different learning strategies will maximize the learning outcomes and long-term retention.(3)
- Educators should encourage the utilization of other learning strategies, such as spacing and reflection, which can be implemented along with interleaving to augment educational tools
- Educators need to always evaluate their instructional approaches, take feedback, and adjust accordingly.
- Presenting the same medical concept in different ways is not interleaving.(18)
- It is helpful to investigate published approaches that have been successfully applied in other institutions and that are in line with the BEME approach and to consider the role you play in contributing to the literature and the generation of evidence.
Student’s perspective:
- Educators can encourage students to mix up their flashcards, question bank exercises, and review topics by grouping things into clusters of topics that, at first glance, may seem difficult to differentiate but whose commonalities will appear through interleaving study. An example is conditions that present similarly.
- Students need to be reminded that interleaving should be done with the goal of learning in mind. For example, if a student is preparing for an internal medicine examination, he/she can interleave between cases of different IM disciplines (cardiology on day 1, then pulmonology on day 2, etc.). If studying for a test on antimicrobials, he/she would need to interleave the different classes of medication.
- Educators should explain why this approach is being used and encouraged. Interleaving takes more effort and is perceived to be more difficult and less rewarding. Making sure students have better metacognition will help them.(19)
Using E-learning Platforms to Make the Most of Interleaving
The role of distributed and distance learning has been thrown into the limelight by the COVID-19 pandemic, but its potential benefits have been previously demonstrated and utilized, even for the implementation of evidence-based learning strategies such as interleaving.(20) E-learning platforms that employ such strategies also play a role in minimizing students’ cognitive biases and improving their metacognition. Content-based learning platforms allow students to access content (or teachers to assign content to students), which can be done in a varied manner, essentially interleaving the exposure to content. Platforms with question banks or clinical cases can also be used to mix up practice instead of solving cases with a blocked approach. Learning platforms should leverage strategies such as interleaving and spaced retrieval, as their implementation within the design of the platform itself can facilitate their application and maximize the impact on students’ learning.
Application of interleaved practice in an online learning platform

Conclusion
Interleaving is a learning strategy that has been demonstrated to improve learning outcomes and long-term retention of knowledge and skills in medical education and other disciplines. As medical education continues to improve by utilizing evidence-based strategies, interleaving should be integrated into school curricula, teaching methodologies, and recommendations for student self-directed learning. More research is needed in order to generate evidence-based guidance. Otherwise, we run the risk of having educators take educated guesses about how to implement interleaving, which can be inaccurate and detrimental when it comes to learning.(21,22) Research must explore the best approaches and how different contexts can be potentiating or limiting factors, while sharing top practices and innovative approaches. With the current available literature, it is clear that medical educators need to implement interleaving into their practice and incorporate other evidence-based strategies to enhance their students’ learning.
Self-Quiz
(Please select all that apply)
1. Which of the following statements are true regarding the definition of interleaving?
a. Interleaving is the act of mixing different but related concepts when learning.
b. Interleaving only works if the concepts can be easily differentiated.
c. Interleaving creates stronger neural links and enhances long-term retention.
d. Interleaving is applicable only for clinical students because they strengthen clinical acumen through patient interactions.
2. Which of the following underlying mechanisms makes interleaving better than blocking for learners?
a. They are able to compare and contrast the different topics and become better at identifying subtle differences.
b. Practicing similar problems causes students to use less cognitive effort.
c. Interleaving adds difficulty that is desirable for learning.
d. Interleaving is a preferred learning strategy among students.
3. What are some examples of ways interleaving can be applied in medical education?
a. In-depth discussion of patient cases and going over different differentials
b. Scheduling of related topics from different disciplines in one study session
c. Teaching pathologies that have similar presentations together
d. Learning about the cardiovascular system through the lens of multiple scientific disciplines
4. What are some key possibilities in the application of interleaving in distance and distributed learning that you feel can be applied in your school?
Correct answers: (1) a, c. (2) a, b, c. (3) a, b, c. (4) free response
Online Seminar
This online seminar from Lecturio’s Durable Learning series explores the concepts of Spacing and Interleaving and how they can provide better long-term learning outcomes. We also share practical recommendations on the integration of Spacing and Interleaving into medical education, both in physical and digital classrooms.
Watch the seminar recording:
Would you like to learn more? Explore the Pulse Seminar Library.


