Urinary incontinence (UI) is the involuntary leakage of urine. It is common, is undertreated, can limit participation in activities, and can impact an individual’s quality of life. In older adults, urinary incontinence can increase overall morbidity and mortality. The 5 types of UI include stress, urge, mixed, overflow, and functional. The etiology of urinary incontinence is often multifactorial. Risk factors for women include prior vaginal deliveries, obesity, and menopause; the leading risk factor for men is previous prostate surgery. Diagnosis is based on clinical history. Testing is individualized to exclude a potentially reversible cause or an underlying medical condition such as infection or malignancy. Management is directed to the type of incontinence and the cause. Treatment most commonly involves lifestyle modification and pelvic floor muscle exercises; some patients may need pharmacologic or surgical treatment. Treatment effectiveness is measured by self-assessment tools.
Urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence (UI) is the involuntary leakage of urine.
Epidemiology[1,3]
Women > men
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency ↑ with age
Both genders are equally affected after 80 years of age.
Globally, approximately 35% of individuals > 60 years of age suffer from UI.
Up to 80% of women in nursing homes have UI.
Only 25% of individuals affected by UI seek treatment owing to social stigma.
Etiology and risk factors[2,4,6,7,20,28]
Age
ObesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity[4]
Major risk factors for women:
History of multiple pregnancies[2]
Current pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
Vaginal delivery
Damage due to surgery or trauma near/on the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess or pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy
MenopauseMenopauseMenopause is a physiologic process in women characterized by the permanent cessation of menstruation that occurs after the loss of ovarian activity. Menopause can only be diagnosed retrospectively, after 12 months without menstrual bleeding. Menopause
Major risk factor for men: prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. surgery
Conditions affecting the brainBrainThe part of central nervous system that is contained within the skull (cranium). Arising from the neural tube, the embryonic brain is comprised of three major parts including prosencephalon (the forebrain); mesencephalon (the midbrain); and rhombencephalon (the hindbrain). The developed brain consists of cerebrum; cerebellum; and other structures in the brain stem.Nervous System: Anatomy, Structure, and Classification or spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy, such as:
Stroke
Multiple sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor
Parkinson diseaseParkinson diseaseParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease
Cerebral palsyPalsyparalysis of an area of the body, thus incapable of voluntary movementCranial Nerve Palsies
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus
Chronic renal disease
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Medications for Parkinson diseaseParkinson diseaseParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease (anticholinergicAnticholinergicAnticholinergic drugs block the effect of the neurotransmitter acetylcholine at the muscarinic receptors in the central and peripheral nervous systems. Anticholinergic agents inhibit the parasympathetic nervous system, resulting in effects on the smooth muscle in the respiratory tract, vascular system, urinary tract, GI tract, and pupils of the eyes. Anticholinergic Drugs)
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation[7]
↑ Alcohol or caffeineCaffeineA methylxanthine naturally occurring in some beverages and also used as a pharmacological agent. Caffeine’s most notable pharmacological effect is as a central nervous system stimulant, increasing alertness and producing agitation. Several cellular actions of caffeine have been observed, but it is not entirely clear how each contributes to its pharmacological profile. Among the most important are inhibition of cyclic nucleotide phosphodiesterases, antagonism of adenosine receptors, and modulation of intracellular calcium handling.Stimulants intake
High impact exercise (jumping and weightlifting)[6]
Consequences of urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence[23,28,29]
Increased:
Rates of depression and social isolation
Hospitalizations
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Pressure ulcers
Admission to long-term residential care
Decreased:
Work productivity
General health
QualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life
Pathophysiology and Classification
Normal bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess function[11,23]
The bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess has 2 main functions:
Store urine (during filling phase)
Expel urine (during voiding phase)
BladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess function is controlled by:
The bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess is innervated by the parasympathetic, sympathetic, and voluntary nervous systems.
During filling → sympathetic stimulation, which leads to:
Contraction of the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric AbscessneckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
Contraction of the external urinary (urethral) sphincter
During voiding:
BladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess distention → activation of mechanoreceptors → afferentAfferentNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology signals to the ponsPonsThe front part of the hindbrain (rhombencephalon) that lies between the medulla and the midbrain (mesencephalon) ventral to the cerebellum. It is composed of two parts, the dorsal and the ventral. The pons serves as a relay station for neural pathways between the cerebellum to the cerebrum.Brain Stem: Anatomy
Inhibition of sympathetic stimulation and relaxation of the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric AbscessneckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
Parasympathetic activation of the detrusor leads to detrusor contraction and the expulsion of urine
Increased intra-abdominal pressure during the Valsalva maneuverValsalva maneuverForced expiratory effort against a closed glottis.Rectal Prolapse is transmitted to the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy (squeezing it closed) and bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess (increasing its pressure) equally, though under normal circumstances, urethral pressure should be enough to maintain continence.
The urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy is supported by the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy muscles, which help to close the urethral opening.
Incontinence pathophysiology and classification[28,29]
Alterations in bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and/or urethral sphincter pressures lead to UI.
Stress urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence (SUI):
Intra-abdominal pressure > bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess sphincter pressure results in urine leakage with effort or exertion (e.g., coughing, running)
No involuntary detrusor contraction
Cause 1: Weakness of the urinary sphincter, which may be from:
Trauma (e.g., during vaginal delivery)
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma therapy
Neurologic disease
Aging
Cause 2: Urethral hypermobility:
Occurs because of damage to the tissue supporting the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy
With this loss of support, during times of ↑ intra-abdominal pressure, the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy moves (rather than being compressed) → results in SUI
Urge urinary incontinence (UUI):
Overactivity of the detrusor muscleDetrusor muscleUrinary Incontinence (called overactive bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess [OAB]) causes an urgency to void and involuntary urine leakage.
An imbalance between stimulatory and inhibitory neural pathways to the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy
Alterations in the sensitivity of detrusor muscleDetrusor muscleUrinary IncontinencereceptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors
Overflow incontinenceOverflow incontinenceSymptom of underactive detrusor muscle of the urinary bladder that contracts with abnormally reduced strength or duration resulting in an incomplete and/or prolonged bladder emptying.Urinary Incontinence:[28]
Incomplete bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess emptying due to:
Inability to void the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess completely → urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium → overdistention of the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess → continuous or frequent loss of urine
Neurologic causes (termed “neurogenic bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess”):
Multiple sclerosisSclerosisA pathological process consisting of hardening or fibrosis of an anatomical structure, often a vessel or a nerve.Wilms Tumor
Spinal cordSpinal cordThe spinal cord is the major conduction pathway connecting the brain to the body; it is part of the CNS. In cross section, the spinal cord is divided into an H-shaped area of gray matter (consisting of synapsing neuronal cell bodies) and a surrounding area of white matter (consisting of ascending and descending tracts of myelinated axons). Spinal Cord: Anatomy injury
Parkinson diseaseParkinson diseaseParkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder. Although the cause is unknown, several genetic and environmental risk factors are currently being studied. Individuals present clinically with resting tremor, bradykinesia, rigidity, and postural instability.Parkinson’s Disease
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus
Enlarged prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid.
Pressure on the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy by a tumorTumorInflammation (e.g., prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. cancer)
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
PregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care
Functional incontinence:
Inability to control urine voiding due to a physical or mental impairment or environmental barriers impeding the individual from reaching the toilet
Not due to lower urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy dysfunction
Common in individuals with dementiaDementiaMajor neurocognitive disorders (NCD), also known as dementia, are a group of diseases characterized by decline in a person’s memory and executive function. These disorders are progressive and persistent diseases that are the leading cause of disability among elderly people worldwide.Major Neurocognitive Disorders, severe arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis, mobility limitationsLimitationsConflict of Interest, or sensorySensoryNeurons which conduct nerve impulses to the central nervous system.Nervous System: Histology impairments
Other types of incontinence classified by the American College of Obstetricians and Gynecologists (ACOG) and the American Urogynecologic Society (AUGS):[29]
Extraurethral urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence, which includes leakage of urine through:
Fistulas (typically to the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy): urethral, vesical, ureteral
Ectopic uretersUretersOne of a pair of thick-walled tubes that transports urine from the kidney pelvis to the urinary bladder.Urinary Tract: Anatomy
Occult stress incontinenceStress incontinenceInvoluntary discharge of urine as a result of physical activities that increase abdominal pressure on the urinary bladder without detrusor contraction or overdistended bladder. The subtypes are classified by the degree of leakage, descent and opening of the bladder neck and urethra without bladder contraction, and sphincter deficiency.Urinary Incontinence: SUI that occurs only after concurrent pelvic organ prolapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse (POP) is reduced (POP may actually “kink” the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy, hiding SUI)
Postural urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence: UI associated with changes in body position
Coital urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence: UI with intercourse
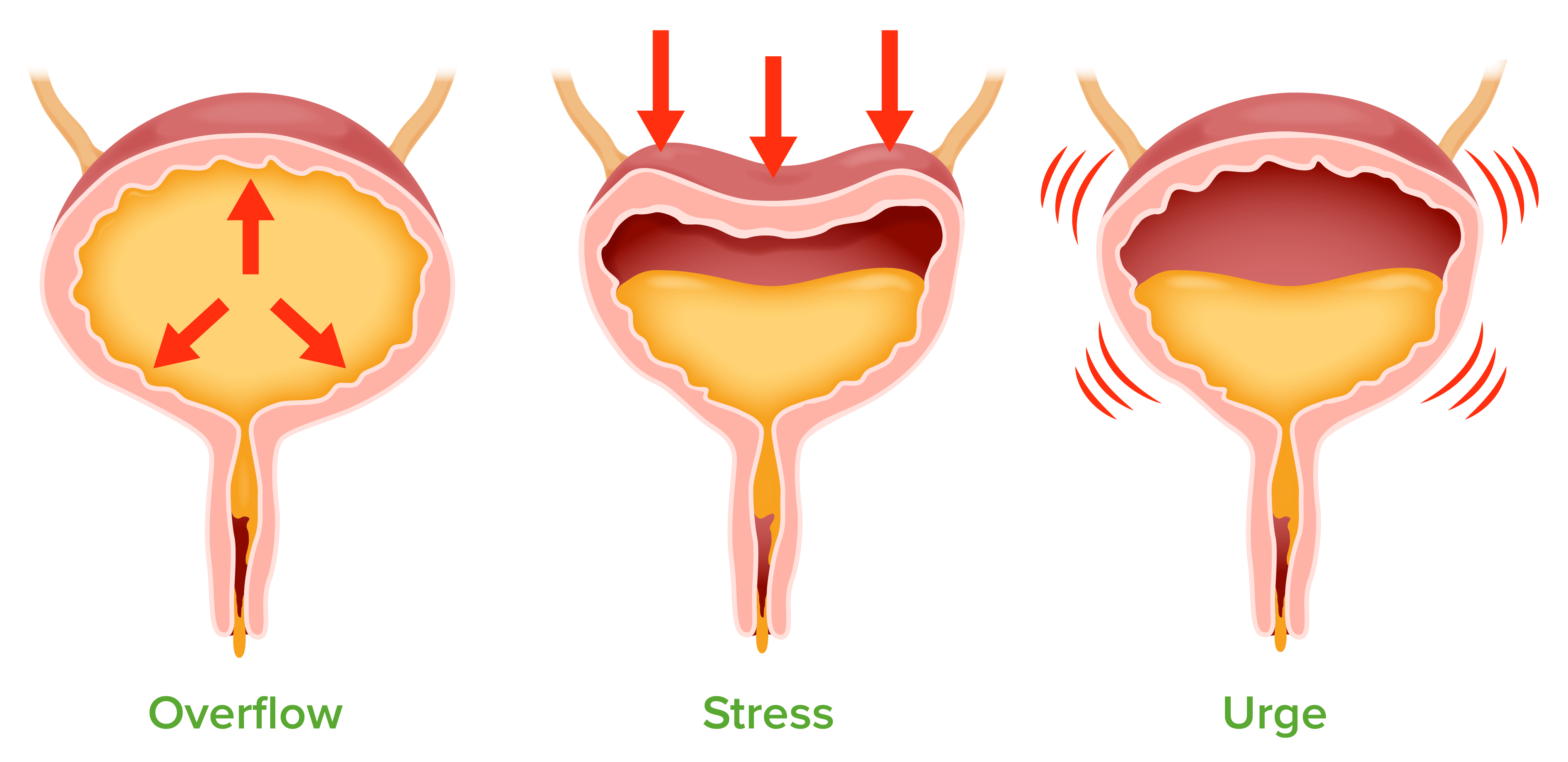
Urinary incontinence:
Overflow: urinary overdistention caused by bladder outlet obstruction or impaired detrusor contractility Stress: urine leakage due to urinary outlet incompetence with increases in intra-abdominal pressure (e.g., coughing, running) Urge: overactivity of the detrusor muscle
Image by Lecturio.
Clinical Presentation and Diagnosis
General approach
Focus the history on symptoms consistent with incontinence based on the type of circumstance:
Diagnosing UI includes:[29,31]
Taking a careful history
Physical exam (which includes a pelvic exam and assessment of urethral mobility)
Attempting to demonstrate SUI
UrinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children
Assessment of post-void residual volumeResidual volumeThe volume of air remaining in the lungs at the end of a maximal expiration. Common abbreviation is rv.Ventilation: Mechanics of Breathing (PVR) and other focused diagnostic testing.
History[18,24-26,29,31]
Take careful history of urinary symptoms:[29]
Characterization of incontinence:
Duration, severity/volume leaked, and effects on daily life
SUI symptoms: UI with increases in intra-abdominal pressure (e.g., during exercise, activity, cough/sneeze)
UUI symptoms: urge to void, but leakage before reaching the restroom
Mixed: symptoms of both
Symptoms related to bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess storage:
↑ Frequency of voiding
NocturiaNocturiaFrequent urination at night that interrupts sleep. It is often associated with outflow obstruction, diabetes mellitus, or bladder inflammation (cystitis).Arginine Vasopressin Disorders (Diabetes Insipidus) or nocturnal enuresisNocturnal enuresisInvoluntary discharge of urine during sleep at night after expected age of completed development of urinary control.Elimination Disorders (leakage of urine when asleep)
Symptoms related to bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess emptying:
Dampness in the undergarments without knowledge of urine leakage
For individuals who have difficulty recalling or quantifying symptoms:
BladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess diary:
Fluid intake
Frequency of voiding
Urine volume
Number of episodes of incontinence
Pad test:
The individual is asked to wear a pad.
The volume of urine leaked is checked by the weight and the number of pads used per day.
Validated UI questionnaires may aid diagnosis/elucidate UI patterns; examples include:[29,30]
Urogenital Distress Inventory (UDI)
Incontinence Impact Questionnaire (IIQ)
Questionnaire for Urinary IncontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence Diagnosis (QUID)
Incontinence QualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of Life Questionnaire (I-QOL)
Incontinence Severity Index (ISI)
International Consultation on Incontinence Questionnaire (ICIQ)
Always ask about impact on qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life:[29]
Disruption in daily activities due to urine leakage
May be a mild nuisance or severely limiting
Asking about the impact of UI will help guide treatment
Comorbid conditions affecting the neurologic system
Alcohol and caffeineCaffeineA methylxanthine naturally occurring in some beverages and also used as a pharmacological agent. Caffeine’s most notable pharmacological effect is as a central nervous system stimulant, increasing alertness and producing agitation. Several cellular actions of caffeine have been observed, but it is not entirely clear how each contributes to its pharmacological profile. Among the most important are inhibition of cyclic nucleotide phosphodiesterases, antagonism of adenosine receptors, and modulation of intracellular calcium handling.Stimulants intake
Medication use
Review of systems:
Infectious causes may present with:
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever/chillsChillsThe sudden sensation of being cold. It may be accompanied by shivering.Fever
Perineal anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts
Integrity and strength of the pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy muscles
Urethral hypermobility:[30]
Defined as ≥ 30 degrees of displacementDisplacementThe process by which an emotional or behavioral response that is appropriate for one situation appears in another situation for which it is inappropriate.Defense Mechanisms from horizontal during Valsalva maneuverValsalva maneuverForced expiratory effort against a closed glottis.Rectal Prolapse while in a supine lithotomy position
Most commonly assessed visually or with the AaAAAmyloidosis point in the Pelvic Organ ProlapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse Quantification (POP-Q) System (used for evaluating pelvic organ prolapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse)
The Q-tip test (a traditional test involving insertion of a Q-tip into the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy) is rarely done any more because it is uncomfortable and has questionable reliabilityReliabilityReliability refers to the reproducibility of a test or research finding.Causality, Validity, and Reliability.
Vaginal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
Pelvic organ prolapsePelvic Organ ProlapsePelvic organ prolapse (POP) is a general term that refers to herniation of 1 or more pelvic organs (e.g., bladder, uterus, rectum) into the vaginal canal, and potentially all the way through the introitus. Weakness and insufficiency of the pelvic floor may result in POP.Pelvic Organ Prolapse
Pelvic/uterine masses
Urethral diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease, which may result in UI episodes or post-void dribbling
FistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula
Attempt to demonstrate SUI: have patient cough or bear down
Abdominal exam to palpate for pelvic and abdominal masses
Rectal exam to check for:
Size and consistencyConsistencyDermatologic Examination of the prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. gland
Stool impaction
Rectal massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
Table: Clinical findings in different types of UI based on office evaluation
Type of UI
History
Possible exam findings
SUI
Leakage of urine due to effort or exertion
When the event causing ↑ intra-abdominal pressure (e.g., coughing) stops, urine leakage stops.
Associated with pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care, childbirth, constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation, and obesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity[4,5,13]
UI demonstrated during Valsalva maneuverValsalva maneuverForced expiratory effort against a closed glottis.Rectal Prolapse on exam (cough stress test)
Urethral hypermobility
Vaginal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation (common after menopauseMenopauseMenopause is a physiologic process in women characterized by the permanent cessation of menstruation that occurs after the loss of ovarian activity. Menopause can only be diagnosed retrospectively, after 12 months without menstrual bleeding. Menopause)
Evidence of trauma/surgery
UUI/OAB
Sudden urge to void immediately (a few seconds) before the involuntary urine leakage starts
Leakage ranges from a few drops to a large amount.
Enlarged prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. in men
Neurologic findings if cause is due to underlying neurologic disease
BladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and/or urethral tenderness if due to underlying cystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs) (+ urinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children findings)
Mixed UI
Characteristics of both SUI and UUI
Findings consistent with both SUI and UUI
Overflow UI
Incomplete bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess emptying
Continuous or frequent loss of urine
Masses that may result in urethral compressionCompressionBlunt Chest Trauma (e.g., pelvic tumorTumorInflammation, enlarged prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid.)
Neurologic symptoms
Functional UI
Presence of cognitive or physical factors impairing the patient’s ability to reach or use the restroom.
Impaired mobility or dexterity
DementiaDementiaMajor neurocognitive disorders (NCD), also known as dementia, are a group of diseases characterized by decline in a person’s memory and executive function. These disorders are progressive and persistent diseases that are the leading cause of disability among elderly people worldwide.Major Neurocognitive Disorders/cognitive impairment
Confusion
Poor eyesight
Extra-urethral UI
Frequent or constant leakage
Often associated with childbirth
FistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula tract may be visible on pelvic exam.
UrinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children:
Blood ureaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea CyclenitrogenNitrogenAn element with the atomic symbol n, atomic number 7, and atomic weight [14. 00643; 14. 00728]. Nitrogen exists as a diatomic gas and makes up about 78% of the earth’s atmosphere by volume. It is a constituent of proteins and nucleic acids and found in all living cells.Urea Cycle
Estimated glomerular filtration rateGlomerular filtration rateThe volume of water filtered out of plasma through glomerular capillary walls into Bowman’s capsules per unit of time. It is considered to be equivalent to inulin clearance.Kidney Function Tests
Clinical tests[26,30,31]
BladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess stress test (also called the “cough stress test”):[30]
Should be done during all UI workups
IIdeally done with a full bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess (at least 300 mL), in order to maximize sensitivity
Ask the individual to cough or bear down.
Observe any urine leakage.
If no urinary leakage is observed, repeat the test with the patient standing.
Interpretation:
Loss of urine during coughing is diagnostic of SUI.
Delayed fluid loss (considered a negative test) suggests detrusor overactivity.
Assess the amount of urine left in the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess after voiding (by ultrasound or straight catheter)
Abnormal: > 150 mL or ⅓ of pre-void volume
Urodynamic tests:
Measure the pressure the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess/urinary sphincter muscle can withstand, and the flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure of urine:
Cystometry: measures pressure and volume of fluid in the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess during filling, storage, and voiding
Uroflowmetry: measures the rate of urine flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure
Urethral pressure profile: tests urethral function
Leak point pressure: determines the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess or abdominal pressure when leakage occurs
Indications:[26,30]
Those with an unclear diagnosis (including a negative cough stress test)
Symptoms that do not correlate with objective findings
Known or suspected neurologic dysfunction
Abnormal urinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children findings (e.g., hematuriaHematuriaPresence of blood in the urine.Renal Cell Carcinoma, pyuriaPyuriaThe presence of white blood cells (leukocytes) in the urine. It is often associated with bacterial infections of the urinary tract. Pyuria without bacteriuria can be caused by tuberculosis, stones, or cancer.Urinary Tract Infections (UTIs))
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with prior pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy or incontinence surgery
Not indicated in cases of uncomplicated SUI, which includes:
SUI demonstrated on cough stress test
Normal urinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children
Indicated based on abnormal history or exam findings
Pelvic ultrasonography:
To detect tumors
To detect nephrolithiasisNephrolithiasisNephrolithiasis is the formation of a stone, or calculus, anywhere along the urinary tract caused by precipitations of solutes in the urine. The most common type of kidney stone is the calcium oxalate stone, but other types include calcium phosphate, struvite (ammonium magnesium phosphate), uric acid, and cystine stones.Nephrolithiasis
To check urine volume before and after voiding
Cystoscopy: A thin tube with a camera is passed through the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy and into the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess.
Abdominal CT: rule out masses/infection (e.g., renal carcinoma, pyelonephritisPyelonephritisPyelonephritis is infection affecting the renal pelvis and the renal parenchyma. This condition arises mostly as a complication of bladder infection that ascends to the upper urinary tract. Pyelonephritis can be acute or chronic (which results from persistent or chronic infections). Typical acute symptoms are flank pain, fever, and nausea with vomiting. TPyelonephritis and Perinephric Abscess)
Management of urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence is often delayed because many individuals hesitate to seek treatment.[9]The major indications for treatment are to treat bothersome symptoms and urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium.
UK guidelines: Urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence in women[18] and men[24]
Factors affecting management
Management of urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence is dependent on several factors:
Type and severity of incontinence
Presence of urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium
Patient preferences:
How bothersome the symptoms are
Desire to try or to avoid certain treatments
Underlying cause
Response to treatment
Age
General health and mental state
Goals of therapy
The major goals of UI therapy are to reduce involuntary leakage and improve qualityQualityActivities and programs intended to assure or improve the quality of care in either a defined medical setting or a program. The concept includes the assessment or evaluation of the quality of care; identification of problems or shortcomings in the delivery of care; designing activities to overcome these deficiencies; and follow-up monitoring to ensure effectiveness of corrective steps.Quality Measurement and Improvement of life. Urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium must be addressed, if present.
Minimize intra-abdominal pressure (through weight lossWeight lossDecrease in existing body weight.Bariatric Surgery, smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases cessation, etcETCThe electron transport chain (ETC) sends electrons through a series of proteins, which generate an electrochemical proton gradient that produces energy in the form of adenosine triphosphate (ATP).Electron Transport Chain (ETC).)
UUI: reduce detrusor overactivity
Overflow incontinenceOverflow incontinenceSymptom of underactive detrusor muscle of the urinary bladder that contracts with abnormally reduced strength or duration resulting in an incomplete and/or prolonged bladder emptying.Urinary Incontinence: address the underlying etiology as much as possible
FistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula/urethral diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease: surgical correction
Note: Catheterization is generally not recommended as part of the management of routine UI. It may be indicated in individuals with persistent urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium, symptomatic infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, and/or renal dysfunction.[31]
Indications for specialist referral[31]
Individuals may need urologic, gynecologic, neurologic, and/or nephrology consultation in the following circumstances:
Recurrent urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: Anatomy infection (UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)) 3 times in 1 year or twice in 6 months; culture-proven
Gross or microscopic hematuriaHematuriaPresence of blood in the urine.Renal Cell Carcinoma in the absence of a UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Lifelong incontinence
Suspected fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula or urethral diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease on pelvic exam
Other abnormal exam findings: uterine prolapseUterine prolapseDownward displacement of the uterus. It is classified in various degrees: in the first degree the uterine cervix is within the vaginal orifice; in the second degree the cervix is outside the orifice; in the third degree the entire uterus is outside the orifice.Pelvic Organ Prolapse, pelvic masses
New neurologic symptoms in addition to UI
Associated fecal incontinenceFecal incontinenceFailure of voluntary control of the anal sphincters, with involuntary passage of feces and flatus.Pediatric Constipation
Suspected overflow incontinenceOverflow incontinenceSymptom of underactive detrusor muscle of the urinary bladder that contracts with abnormally reduced strength or duration resulting in an incomplete and/or prolonged bladder emptying.Urinary Incontinence/urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium
Lifestyle and behavioral modifications, including pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy muscle exercises, are 1st-line therapy for all types of UI in both men and women.
Weight lossWeight lossDecrease in existing body weight.Bariatric Surgery in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with obesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity[4,5,13,29]
Management of constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
Dietary changes:
Reduce or eliminate bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess irritants: alcohol, caffeineCaffeineA methylxanthine naturally occurring in some beverages and also used as a pharmacological agent. Caffeine’s most notable pharmacological effect is as a central nervous system stimulant, increasing alertness and producing agitation. Several cellular actions of caffeine have been observed, but it is not entirely clear how each contributes to its pharmacological profile. Among the most important are inhibition of cyclic nucleotide phosphodiesterases, antagonism of adenosine receptors, and modulation of intracellular calcium handling.Stimulants, vitamin CVitamin CA six carbon compound related to glucose. It is found naturally in citrus fruits and many vegetables. Ascorbic acid is an essential nutrient in human diets, and necessary to maintain connective tissue and bone. Its biologically active form, vitamin C, functions as a reducing agent and coenzyme in several metabolic pathways. Vitamin C is considered an antioxidant.Water-soluble Vitamins and their Deficiencies, and carbonated beverages
Normalize fluid intake if drinking excess amounts of water; limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation fluid to 2 L per day.[29]
Avoid drinking water for several hours before bedtime.
SmokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases cessation
Timed voiding and bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess training: urinate on a schedule; start by voiding every 30‒60 minutes
Urinate before physical or strenuous activities.
Do not wait for the urge to urinate.
The time between trips to the bathroom is progressively delayed.
Gradually ↑ time between voids to 2.5–3.5 hours as tolerated.
Double voiding: Avoid overflow incontinenceOverflow incontinenceSymptom of underactive detrusor muscle of the urinary bladder that contracts with abnormally reduced strength or duration resulting in an incomplete and/or prolonged bladder emptying.Urinary Incontinence by urinating and then urinating again after a few minutes.
Avoid ↑ intra-abdominal pressure maneuvers (e.g., heavy lifting)
Pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy muscle (Kegel) exercises:[15,18,29]
Effective in stress and urge incontinenceUrge incontinenceInvoluntary discharge of urine that is associated with an abrupt and strong desire to void. It is usually related to the involuntary contractions of the detrusor muscle of the bladder (detrusor hyperreflexia or detrusor instability).Urinary Incontinence
Supervised pelvic floorPelvic floorSoft tissue formed mainly by the pelvic diaphragm, which is composed of the two levator ani and two coccygeus muscles. The pelvic diaphragm lies just below the pelvic aperture (outlet) and separates the pelvic cavity from the perineum. It extends between the pubic bone anteriorly and the coccyx posteriorly.Vagina, Vulva, and Pelvic Floor: Anatomy muscle training (PFMT) with a trained clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship/physiotherapist is highly recommended to learn proper technique and improve outcomes.
Similar in both men and women:
Contract the muscles that are used to stop the flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressure of urine for 5 seconds.
Relax the muscles for the next 5 seconds.
Note: PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should not do KegelsKegelsUrinary Incontinence while actually urinating (except for maybe the 1st time or 2 in order to learn which muscles to contract).
Effort should be made to progress gradually to 10 seconds per contraction.
3 sets of repetitions per day
Symptom management with pads or moisture-wicking catheters
Management of SUI in women[17,28,29]
In addition to the behavior/lifestyle interventions mentioned above, nonsurgical (conservative) and surgical options exist for female patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with SUI who desire additional therapy.
Nonsurgical options:[28,29]
Vaginal estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy:
For perimenopausal and postmenopausal women with vaginal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
Tones and rejuvenates urethral and vaginal tissues
Preparations:
EstradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins vaginal cream (100 µg estradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins per 1 g of cream): Insert 0.5–1 g of cream intravaginally daily for 2 weeks and then 0.5 mg–1 g twice weekly.
EstradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins vaginal tablet/inserts (Imvexxy®, Vagifem®, Yuvafem®): Insert 4- or 10-µg tablet intravaginally once daily for 2 weeks and then twice weekly.
EstradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins ring (Estring®): 2-mg intravaginal ring (releases 7.5 µg estradiolEstradiolThe 17-beta-isomer of estradiol, an aromatized C18 steroid with hydroxyl group at 3-beta- and 17-beta-position. Estradiol-17-beta is the most potent form of mammalian estrogenic steroids.Noncontraceptive Estrogen and Progestins per day); replace every 90 days
Note: Systemic estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy does not improve SUI symptoms.[28]
Continence pessary:
A flexible silicone device that is inserted into the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy; provides support for the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy
Available in a variety of shapes and sizes
Some pessariesPessariesDevices worn in the vagina to provide support to displaced uterus or rectum. Pessaries are used in conditions such as uterine prolapse; cystocele; or rectocele.Pelvic Organ Prolapse also support the internal pelvic organs and are used to treat POP as well.
Must be fitted by a clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship in clinic
Instructions for use:
Inserted and removed by the patient; worn as needed
Wash with soap and water when removed
For frequent SUI symptoms: typically inserted during the day and removed at night
May be inserted by clinicianClinicianA physician, nurse practitioner, physician assistant, or another health professional who is directly involved in patient care and has a professional relationship with patients.Clinician–Patient Relationship in clinic and left in place for up to 3 months at a time if the patient is unable to remove and replace the device herself
Concurrent vaginal estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy may help reduce vaginal atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation and the risk of erosionErosionPartial-thickness loss of the epidermisGeneralized and Localized Rashes
Vaginal inserts (e.g., Poise® Impressa®):
A tampon-like device inserted into the vaginaVaginaThe vagina is the female genital canal, extending from the vulva externally to the cervix uteri internally. The structures have sexual, reproductive, and urinary functions and a rich blood supply, mainly arising from the internal iliac artery.Vagina, Vulva, and Pelvic Floor: Anatomy that functions like a pessary, supporting the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy
Available over the counter without a prescription
DuloxetineDuloxetineA thiophene derivative and selective neurotransmitter uptake inhibitor for serotonin and noradrenaline (SNRI). It is an antidepressant agent and anxiolytic, and is also used for the treatment of pain in patients with diabetes mellitus and fibromyalgia.Serotonin Reuptake Inhibitors and Similar Antidepressants:[28]
Approved for SUI in Europe (off-label in the US)
A serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS–norepinephrineNorepinephrinePrecursor of epinephrine that is secreted by the adrenal medulla and is a widespread central and autonomic neurotransmitter. Norepinephrine is the principal transmitter of most postganglionic sympathetic fibers, and of the diffuse projection system in the brain that arises from the locus ceruleus.Receptors and Neurotransmitters of the CNS reuptake inhibitor (SNRI)
Acts on the pudendal nervePudendal nerveA nerve which originates in the sacral spinal cord (s2 to s4) and innervates the perineum, the external genitalia, the external anal sphincter and the external urethral sphincter. It has three major branches: the perineal nerve, inferior anal nerves, and the dorsal nerve of penis or clitoris.Gluteal Region: Anatomy alpha-adrenergic and 5-hydroxytryptamine-2 receptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors, which may improve urinary symptoms
Dose: 20–40 mg once or twice daily (start with lower dose)
Surgical options:[17,28,29]
Urethral bulking agents:
Synthetic bulking material is injected into the tissue surrounding the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy.
Increased mechanical pressure around the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy prevents leaking.
Materials:
Solid silicone elastomer (Macroplastique®)
Hydrogel (Bulkamid®)
Glutaraldehyde cross-linked collagenCollagenA polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth).Connective Tissue: Histology (Contigent®)
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes hydroxyapatite (Coaptite®)
Less effective than other surgical options, may require repeat injections
Mid-urethral slings (MUS):
Synthetic mesh creates a sling under the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy at the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric AbscessneckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess.
Highest success rates of all available SUI interventions
Most commonly used surgical intervention
Procedures (equivalent efficacy):
Transvaginal tape (TVT): edges/sides of the sling are retropubic; higher risk of bladder perforationBladder PerforationBasic Procedures and postoperative voiding dysfunction
Transobturator tape (TOT): edges/sides are through the obturator foramen; higher risk of postoperative groinGroinThe external junctural region between the lower part of the abdomen and the thigh.Male Genitourinary ExaminationpainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Autologous fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis pubovaginal sling
FasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis is typically from the rectus sheath or fascia lataFascia lataFemoral Region and Hernias: Anatomy
More effective than colposuspension procedure
Burch (retropubic) colposuspension: traditional procedure; higher risk of voiding difficulties postoperatively than with MUS
Management of SUI in men[24]
After lifestyle/behavioral interventions, the most common management techniques include:
DuloxetineDuloxetineA thiophene derivative and selective neurotransmitter uptake inhibitor for serotonin and noradrenaline (SNRI). It is an antidepressant agent and anxiolytic, and is also used for the treatment of pain in patients with diabetes mellitus and fibromyalgia.Serotonin Reuptake Inhibitors and Similar Antidepressants (approved in Europe, off-label in the US)
Transurethral bulking agents:
Lower success rates than in women; typically < 25%
Typically requires repeated injections
Perineal sling:
Use synthetic mesh placed through the obturator foramen.
Typically for postprostatectomy SUI, if symptoms do not resolve spontaneously after 6‒12 months of observation
Artificial urinary sphincter:
Most effective long-term treatment for severe SUI
A fluid- or air-filled ring is placed around the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy, acting as an artificial sphincter when the cuff is inflated.
A pumpPumpACES and RUSH: Resuscitation Ultrasound Protocols is implanted under the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions in the scrotumScrotumA cutaneous pouch of skin containing the testicles and spermatic cords.Testicles: Anatomy, which moves the fluid or air in the cuff to a reservoirReservoirAnimate or inanimate sources which normally harbor disease-causing organisms and thus serve as potential sources of disease outbreaks. Reservoirs are distinguished from vectors (disease vectors) and carriers, which are agents of disease transmission rather than continuing sources of potential disease outbreaks. Humans may serve both as disease reservoirs and carriers.Escherichia coli/balloon located in the abdominal cavity when the patient needs to void.
Management of UUI and OAB in women
In UUI/OAB, medical management with antimuscarinic agents or β3-adrenergic agonists are the mainstay of initial therapy after behavior/lifestyle interventions. If pharmacologic therapy is inadequate, additional treatment options are available.
Trospium (taken on an empty stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy):
SolifenacinSolifenacinA quinuclidine and tetrahydroisoquinoline derivative and selective m3 muscarinic antagonist. It is used as a urologic agent in the treatment of urinary incontinence.Anticholinergic Drugs 5–10 mg once daily
TolterodineTolterodineAn antimuscarinic agent selective for the muscarinic receptors of the bladder that is used in the treatment of urinary incontinence and urinary urge incontinence.Anticholinergic Drugs:
Extended-release 2–4 mg once daily
Immediate-release 1–2 mg twice daily
Potential adverse effects: peripheral anticholinergicAnticholinergicAnticholinergic drugs block the effect of the neurotransmitter acetylcholine at the muscarinic receptors in the central and peripheral nervous systems. Anticholinergic agents inhibit the parasympathetic nervous system, resulting in effects on the smooth muscle in the respiratory tract, vascular system, urinary tract, GI tract, and pupils of the eyes. Anticholinergic Drugs effects
Urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium
Dry mouth and dry eyes
ConstipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
GI upset
Somnolence
Mental status changes/decreased cognitive function, primarily in older adults
ContraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation to antimuscarinic drugs:
Tachyarrhythmias
Myasthenia gravisMyasthenia GravisMyasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by weakness and fatigability of skeletal muscles caused by dysfunction/destruction of acetylcholine receptors at the neuromuscular junction. MG presents with fatigue, ptosis, diplopia, dysphagia, respiratory difficulties, and progressive weakness in the limbs, leading to difficulty in movement. Myasthenia Gravis
Stimulate bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric AbscessreceptorsReceptorsReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors, triggering smooth muscle relaxation
Have similar efficacy to and fewer potential adverse effects than antimuscarinic agents
Avoid in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with uncontrolled hypertensionUncontrolled hypertensionAlthough hypertension is defined as a blood pressure of > 130/80 mm Hg, individuals can present with comorbidities of severe asymptomatic or “uncontrolled” hypertension (≥ 180 mm Hg systolic and/or ≥ 120 mm Hg diastolic) that carries with it a significant risk of morbidity and mortality. Uncontrolled Hypertension
Monitor blood pressure after starting.
Vibegron: 75 mg daily
Potential adverse effects:
Urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium
HypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension with mirabegron
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
Additional treatment options[28,29] (for individuals whose symptoms were not adequately controlled by, or who could not tolerate, antimuscarinic and β-adrenergic agents):
Tibial nerveTibial NerveThe medial terminal branch of the sciatic nerve. The tibial nerve fibers originate in lumbar and sacral spinal segments (L4 to S2). They supply motor and sensory innervation to parts of the calf and foot.Popliteal Fossa: Anatomy stimulation:[28]
Percutaneous or transcutaneous electrical stimulation of the posterior tibial nerveTibial NerveThe medial terminal branch of the sciatic nerve. The tibial nerve fibers originate in lumbar and sacral spinal segments (L4 to S2). They supply motor and sensory innervation to parts of the calf and foot.Popliteal Fossa: Anatomy just above the medial ankle
Typical treatment cycle: 30-minute sessions once a week for 12 weeks
Injection of botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism(neurotoxin inhibiting the presynaptic release of acetylcholineAcetylcholineA neurotransmitter found at neuromuscular junctions, autonomic ganglia, parasympathetic effector junctions, a subset of sympathetic effector junctions, and at many sites in the central nervous system.Receptors and Neurotransmitters of the CNS:[29]
May lead to bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess paralysis and higher rates of UTIUTIUrinary tract infections (UTIs) represent a wide spectrum of diseases, from self-limiting simple cystitis to severe pyelonephritis that can result in sepsis and death. Urinary tract infections are most commonly caused by Escherichia coli, but may also be caused by other bacteria and fungi. Urinary Tract Infections (UTIs)
Sacral neuromodulation (InterStim®):[29]
Beneficial primarily for OAB and neurogenic incontinence
Device is inserted subcutaneously in the buttock, with electrodesElectrodesElectric conductors through which electric currents enter or leave a medium, whether it be an electrolytic solution, solid, molten mass, gas, or vacuum.Electrocardiogram (ECG) placed near the sacral nerve
Delivers an electric signal that stimulates the sacral nerve and aids in bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess control
High rate of reintervention within 5 years due to device malfunction
Management of UUI/OAB in men[24,25]
As in women, primary management of UUI/OAB in men is with pharmacologic agents. Additional options exist for those for whom medical management fails.
Medications:
Antimuscarinic anticholinergicsAnticholinergicsAnticholinergic drugs block the effect of the neurotransmitter acetylcholine at the muscarinic receptors in the central and peripheral nervous systems. Anticholinergic agents inhibit the parasympathetic nervous system, resulting in effects on the smooth muscle in the respiratory tract, vascular system, urinary tract, GI tract, and pupils of the eyes. Anticholinergic Drugs:
Use with caution in benignBenignFibroadenoma prostatic hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation (BPHBPHBenign prostatic hyperplasia (bph) is a condition indicating an increase in the number of stromal and epithelial cells within the prostate gland (transition zone). Benign prostatic hyperplasia is common in men > 50 years of age and may greatly affect their quality of life.Benign Prostatic Hyperplasia; especially when PVRs are ≥ 250 mL) in order to avoid worsening urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium.
Typically 2nd-line, behind antimuscarinic anticholinergicsAnticholinergicsAnticholinergic drugs block the effect of the neurotransmitter acetylcholine at the muscarinic receptors in the central and peripheral nervous systems. Anticholinergic agents inhibit the parasympathetic nervous system, resulting in effects on the smooth muscle in the respiratory tract, vascular system, urinary tract, GI tract, and pupils of the eyes. Anticholinergic Drugs
Less concern about urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium than with anticholinergicsAnticholinergicsAnticholinergic drugs block the effect of the neurotransmitter acetylcholine at the muscarinic receptors in the central and peripheral nervous systems. Anticholinergic agents inhibit the parasympathetic nervous system, resulting in effects on the smooth muscle in the respiratory tract, vascular system, urinary tract, GI tract, and pupils of the eyes. Anticholinergic Drugs
Same drugs/dosing as for women (mirabegron, vibegron)
α1-Adrenergic receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonists:
Helpful for UI due to prostatic enlargement in men with BPHBPHBenign prostatic hyperplasia (bph) is a condition indicating an increase in the number of stromal and epithelial cells within the prostate gland (transition zone). Benign prostatic hyperplasia is common in men > 50 years of age and may greatly affect their quality of life.Benign Prostatic Hyperplasia and bladder outlet obstructionBladder Outlet ObstructionBenign Prostatic Hyperplasia
Function to relax the smooth muscle toneMuscle toneThe state of activity or tension of a muscle beyond that related to its physical properties, that is, its active resistance to stretch. In skeletal muscle, tonus is dependent upon efferent innervation.Skeletal Muscle Contraction of the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric AbscessneckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
Usually used in combination with other agents
Oral drugs (start with the lowest dose):
DoxazosinDoxazosinA prazosin-related compound that is a selective alpha-1-adrenergic blocker.Antiadrenergic Drugs 1–8 mg once daily
TamsulosinTamsulosinA sulfonamide derivative and adrenergic alpha-1 receptor antagonist that is used to relieve symptoms of urinary obstruction caused by benign prostatic hyperplasia.Antiadrenergic Drugs 0.4 mg once daily
Helpful for UI due to prostatic enlargement in men with BPHBPHBenign prostatic hyperplasia (bph) is a condition indicating an increase in the number of stromal and epithelial cells within the prostate gland (transition zone). Benign prostatic hyperplasia is common in men > 50 years of age and may greatly affect their quality of life.Benign Prostatic Hyperplasia
Often used in combination
Oral drugs:
FinasterideFinasterideAn orally active 3-oxo-5-alpha-steroid 4-dehydrogenase inhibitor. It is used as a surgical alternative for treatment of benign prostatic hyperplasia.Androgens and Antiandrogens 5 mg once daily
DutasterideDutasterideA 5-alpha-reductase inhibitor that is reported to inhibit both type-1 and type 2 isoforms of the enzyme and is used to treat benign prostatic hyperplasia.Androgens and Antiandrogens 0.5 mg once daily
Botulinum toxinBotulinum toxinToxic proteins produced from the species Clostridium botulinum. The toxins are synthesized as a single peptide chain which is processed into a mature protein consisting of a heavy chain and light chain joined via a disulfide bond. The botulinum toxin light chain is a zinc-dependent protease which is released from the heavy chain upon endocytosis into presynaptic nerve endings. Once inside the cell the botulinum toxin light chain cleaves specific snare proteins which are essential for secretion of acetylcholine by synaptic vesicles. This inhibition of acetylcholine release results in muscular paralysis.Botulism: for refractory symptoms
Tibial nerveTibial NerveThe medial terminal branch of the sciatic nerve. The tibial nerve fibers originate in lumbar and sacral spinal segments (L4 to S2). They supply motor and sensory innervation to parts of the calf and foot.Popliteal Fossa: Anatomy stimulation: for refractory symptoms
Suitable for light-to-moderate cases to prevent leakage of urine
Short-term use
Catheterization:
Generally not recommended to manage UI symptoms
Indicated in individuals unable to empty their bladders and/or with urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium
Procedural options:
Typical indications:
Bladder outlet obstructionBladder Outlet ObstructionBenign Prostatic Hyperplasia/enlarged prostateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. with urinary retentionUrinary retentionInability to empty the urinary bladder with voiding (urination).Delirium
Failed medical management
Treatments for BPHBPHBenign prostatic hyperplasia (bph) is a condition indicating an increase in the number of stromal and epithelial cells within the prostate gland (transition zone). Benign prostatic hyperplasia is common in men > 50 years of age and may greatly affect their quality of life.Benign Prostatic Hyperplasia include:
ProstateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. ablation: vaporization, laser, microwave
ProstateProstateThe prostate is a gland in the male reproductive system. The gland surrounds the bladder neck and a portion of the urethra. The prostate is an exocrine gland that produces a weakly acidic secretion, which accounts for roughly 20% of the seminal fluid. resection
Sacral neuromodulation:
Same procedure as in women (most studies with this technology are in women)
Candidates: men with refractory symptoms
Billing and Coding
Diagnosis Codes:
These codes are used to specify the type of urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence, such as stress incontinenceStress incontinenceInvoluntary discharge of urine as a result of physical activities that increase abdominal pressure on the urinary bladder without detrusor contraction or overdistended bladder. The subtypes are classified by the degree of leakage, descent and opening of the bladder neck and urethra without bladder contraction, and sphincter deficiency.Urinary Incontinence (leakage with cough/sneeze), urge incontinenceUrge incontinenceInvoluntary discharge of urine that is associated with an abrupt and strong desire to void. It is usually related to the involuntary contractions of the detrusor muscle of the bladder (detrusor hyperreflexia or detrusor instability).Urinary Incontinence (sudden, intense urge), or mixed types.
Coding System
Code
Description
ICD-10-CM
N39.3
Stress incontinenceStress incontinenceInvoluntary discharge of urine as a result of physical activities that increase abdominal pressure on the urinary bladder without detrusor contraction or overdistended bladder. The subtypes are classified by the degree of leakage, descent and opening of the bladder neck and urethra without bladder contraction, and sphincter deficiency.Urinary Incontinence (female) (male)
ICD-10-CM
N39.41
Urge incontinenceUrge incontinenceInvoluntary discharge of urine that is associated with an abrupt and strong desire to void. It is usually related to the involuntary contractions of the detrusor muscle of the bladder (detrusor hyperreflexia or detrusor instability).Urinary Incontinence
ICD-10-CM
N39.46
Mixed incontinence
ICD-10-CM
R32
Unspecified urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence
Evaluation & Workup:
These codes are used for the diagnostic workup, which includes a basic urinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children to rule out infection and complex urodynamic studies to assess bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess and sphincter function in detail.
Coding System
Code
Description
CPT
81001
UrinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children, by dip stick or tablet reagent
This CPT code is for a sling operation, a common and effective surgical procedure for treating female stress urinary incontinenceUrinary incontinenceUrinary incontinence (UI) is involuntary loss of bladder control or unintentional voiding, which represents a hygienic or social problem to the patient. Urinary incontinence is a symptom, a sign, and a disorder. The 5 types of UI include stress, urge, mixed, overflow, and functional.Urinary Incontinence by providing support to the urethraUrethraA tube that transports urine from the urinary bladder to the outside of the body in both the sexes. It also has a reproductive function in the male by providing a passage for sperm.Urinary Tract: Anatomy.
Coding System
Code
Description
CPT
57288
Sling operation for stress incontinenceStress incontinenceInvoluntary discharge of urine as a result of physical activities that increase abdominal pressure on the urinary bladder without detrusor contraction or overdistended bladder. The subtypes are classified by the degree of leakage, descent and opening of the bladder neck and urethra without bladder contraction, and sphincter deficiency.Urinary Incontinence (eg, fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis or synthetic)
Medications:
These codes are for medications used to treat urge incontinenceUrge incontinenceInvoluntary discharge of urine that is associated with an abrupt and strong desire to void. It is usually related to the involuntary contractions of the detrusor muscle of the bladder (detrusor hyperreflexia or detrusor instability).Urinary Incontinence. AnticholinergicsAnticholinergicsAnticholinergic drugs block the effect of the neurotransmitter acetylcholine at the muscarinic receptors in the central and peripheral nervous systems. Anticholinergic agents inhibit the parasympathetic nervous system, resulting in effects on the smooth muscle in the respiratory tract, vascular system, urinary tract, GI tract, and pupils of the eyes. Anticholinergic Drugs like oxybutyninOxybutyninAnticholinergic Drugs relax the bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess muscle, while beta-3 agonists like mirabegron also help increase bladderBladderA musculomembranous sac along the urinary tract. Urine flows from the kidneys into the bladder via the ureters, and is held there until urination.Pyelonephritis and Perinephric Abscess capacity.
Patel, U. J., Godecker, A. L., Giles, D. L., Brown, H. W. (2022). Updated prevalence of urinary incontinence in women: 2015-2018 national population-based survey data. Female Pelvic Medicine & Reconstructive Surgery, 28(4), 181–7. doi: 10.1097/SPV.0000000000001127
Wuytack, F., Moran, P., Daly, D., Begley, C. (2022). Is there an association between parity and urinary incontinence in women during pregnancy and the first year postpartum? A systematic review and meta-analysis. Neurourology and Urodynamics, 41(1), 54–90. doi: 10.1002/nau.24785
Lee, U. J., Feinstein, L., Ward, J. B., Kirkali, Z., Martinez-Miller, E. E., Matlaga, B. R., Kobashi, K. C. (2021). Prevalence of urinary incontinence among a nationally representative sample of women, 2005-2016: findings from the Urologic Diseases in America Project. Journal of Urology, 205(6), 1718–1724. doi: 10.1097/JU.0000000000001634
Marcelissen, T., Anding, R., et al. (2019). Exploring the relation between obesity and urinary incontinence: pathophysiology, clinical implications, and the effect of weight reduction, ICI–RS 2018. Neurourology and Urodynamics, 38(Suppl 5), S18–S24. doi: 10.1002/nau.24072
Sheridan, W., Da Silva, A.S., et al. (2021). Weight loss with bariatric surgery or behaviour modification and the impact on female obesity-related urine incontinence: a comprehensive systematic review and meta-analysis. Clinical Obesity, 11(4), e12450. doi: 10.1111/cob.12450
Elks, W., Jaramillo-Huff, A., Barnes, K.L., Petersen, T. R., Komesu, Y. M. (2020). The Stress Urinary Incontinence in CrossFit (SUCCeSS) Study. Female Pelvic Medicine & Reconstructive Surgery, 26(2), 101–106. doi: 10.1097/SPV.0000000000000815
Lian, W. Q., Li, F. J., Huang, H. X., Zheng, Y. Q., Chen, L. H. (2019). Constipation and risk of urinary incontinence in women: a meta-analysis. International Urogynecology Journal, 30(10), 1629–1634. doi: 10.1007/s00192-019-03941-w
Alexander, J. W., et al. (2022). CO2 surgical laser for treatment of stress urinary incontinence in women: a randomized controlled trial. American Journal of Obstetrics and Gynecology, 227(3), 473.e1-473.e12. doi: 10.1016/j.ajog.2022.05.054
Jarbøl, D. E., Haastrup, P. F., et al. (2021). Women’s barriers for contacting their general practitioner when bothered by urinary incontinence: a population-based cross-sectional study. BMC Urology, 21(1), 99. doi: 10.1186/s12894-021-00864-x
Uhr, A., Glick, L., Barron, S., et al. (2021). How I do it: PureWick female external catheter: a non-invasive urine management system for incontinent women. Canadian Journal of Urology, 28(3), 10669–10672. https://pubmed.ncbi.nlm.nih.gov/34129459/
Vo, A., Kielb, S. J. (2018). Female voiding dysfunction and urinary incontinence. Medical Clinics of North America, 102(2), 313–324. doi: 10.1016/j.mcna.2017.10.006
Balk, E. M., Rofeberg, V. N., Adam, G. P., Kimmel, H. J., Trikalinos, T. A., Jeppson, P. C. (2019). Pharmacologic and nonpharmacologic treatments for urinary incontinence in women: a systematic review and network meta-analysis of clinical outcomes. Annals of Internal Medicine, 170(7), 465–479. doi: 10.7326/M18-3227
Yazdany, T., Jakus-Waldman, S., et al. (2020). American Urogynecologic Society systematic review: the impact of weight loss intervention on lower urinary tract symptoms and urinary incontinence in overweight and obese women. Female pelvic Medicine & Reconstructive Surgery, 26(1), 16–29. doi: 10.1097/SPV.0000000000000802
Huang, A. J. (2013). Nonsurgical treatments for urinary incontinence in women: summary of primary findings and conclusions. JAMA Internal Medicine, 173(15), 1463–1464. doi: 10.1001/jamainternmed.2013.7818
Dumoulin, C., Cacciari, L. P., Hay-Smith, E. J. C. (2018). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews, 10, CD005654. doi: 10.1002/14651858.CD005654.pub4
Imamura, M., Hudson, J., et al. (2019). Surgical interventions for women with stress urinary incontinence: systematic review and network meta-analysis of randomised controlled trials. BMJ, 365, l1842. doi: 10.1136/bmj.l1842
Hoe, V., Haller, B., Yao, H.H., & O’Connell, H.E. (2021). Urethral bulking agents for the treatment of stress urinary incontinence in women: a systematic review. Neurourology and Urodynamics, 40(6), 1349–1388. doi: 10.1002/nau.24696
National Institute for Health and Care Excellence (NICE). (2021). Quality standard on urinary incontinence in women. Retrieved August 31, 2022, from https://www.nice.org.uk/guidance/qs77
Downey, A., Inman, R. D. (2019). Recent advances in surgical management of urinary incontinence. F1000Research, 8(F1000 Faculty Rev),1294. doi: 10.12688/f1000research.16356.1
Irwin, G. M. (2019). Urinary incontinence. Primary Care, 46(2), 233–42. doi: 10.1016/j.pop.2019.02.004
Lightner, D. J., Gomelsky, A., Souter, L., Vasavada, S. P. (2019). Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline amendment 2019. Journal of Urology, 202(3), 558–563. doi: 10.1097/JU.0000000000000309
Kobashi, K. C., et al. (2017). Surgical treatment of female stress urinary incontinence (SUI): AUA/SUFU guideline. Journal of Urology, 198(4), 875–883. doi: 10.1016/j.juro.2017.06.061
Lightner, D. J., Gomelsky, A., Souter, L., Vasavada, S. P. (2019). Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline amendment 2019. Journal of Urology, 202, 558–563. https://doi.org/10.1097/JU.0000000000000309
Harding, C. K., Lapitan, M.C., Arlandis, S., et al. (2022). EAU guidelines on management of non-neurogenic female lower urinary tract symptoms. European Association of Urology. Retrieved Jan 20, 2026, from https://uroweb.org/guidelines/non-neurogenic-female-luts
American College of Obstetricians and Gynecologists Committee on Practice Bulletins – Gynecology & The American Urogynecologic Society. (2015). Practice Bulletin No. 155: Urinary incontinence in women. Obstetrics & Gynecology, 126(5), e66‒e81. doi: 10.1097/AOG.0000000000001148
American Urogynecologic Society Committee on Gynecologic Practice. (2014). Committee opinion no. 603: evaluation of uncomplicated stress urinary incontinence in women before surgical treatment. Obstetrics & Gynecology, 123(6), 1403‒1407. https://doi.org/10.1097/01.AOG.0000450759.34453.31