Rhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation. Rhabdomyolysis can result from trauma or direct muscle injuries; however, non-exertional and non-traumatic etiologies (heatstroke, immobilization, medication side effects) can also lead to muscle breakdown. The classic triad of symptoms includes myalgia, weakness, and tea-colored urine, but the presentation can be nonspecific. The diagnosis is clinical, based on history, exam, and lab findings, typically including elevated creatine kinase levels, abnormal electrolytes with possible renal failure, and dark urine without RBCs (indicating myoglobinuria). Management of rhabdomyolysis involves aggressive IV fluid resuscitation and appropriately managing electrolyte abnormalities, triggering events, and acute kidney injury (if present).
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis is a syndrome marked by muscle necrosisMuscle NecrosisRhabdomyolysis, resulting in the release of toxic intracellular muscle constituents into the circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment (especially myoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis).
Acute lower-limb compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome
Exertion occurring in extremely hot or humid conditions (heatstrokeHeatstrokeHeatstroke is an illness characterized as a core body temperature exceeding 40°C (104°F) with accompanying neurological symptoms including ataxia, seizures, and/or delirium. Heatstroke is usually due to the body’s inability to regulate its temperature when challenged with an elevated heat load. Heatstroke)
Seizure
Non-exertional and non-traumatic rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis:
Alcohol, use of illicit drugsIllicit DrugsDrugs that are manufactured, obtained, or sold illegally. They include prescription drugs obtained or sold without prescription and non-prescription drugs. Illicit drugs are widely distributed, tend to be grossly impure and may cause unexpected toxicity.Delirium
Drugs (e.g., statinsStatinsStatins are competitive inhibitors of HMG-CoA reductase in the liver. HMG-CoA reductase is the rate-limiting step in cholesterol synthesis. Inhibition results in lowered intrahepatocytic cholesterol formation, resulting in up-regulation of LDL receptors and, ultimately, lowering levels of serum LDL and triglycerides.Statins, colchicineColchicineA major alkaloid from colchicum autumnale l. And found also in other colchicum species. Its primary therapeutic use is in the treatment of gout.Gout Drugs)
Metabolic disorders and abnormalities (e.g., inherited disorders of glycogenolysisGlycogenolysisThe release of glucose from glycogen by glycogen phosphorylase (phosphorolysis). The released glucose-1-phosphate is then converted to glucose-6-phosphate by phosphoglucomutase before entering glycolysis. Glycogenolysis is stimulated by glucagon or epinephrine via the activation of phosphorylase kinase.Glycogen Metabolism)
Electrolyte abnormalities (e.g., hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia)
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., viral infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease)
Toxins (e.g., carbon monoxideCarbon monoxideCarbon monoxide (CO). A poisonous colorless, odorless, tasteless gas. It combines with hemoglobin to form carboxyhemoglobin, which has no oxygen carrying capacity. The resultant oxygen deprivation causes headache, dizziness, decreased pulse and respiratory rates, unconsciousness, and death.Carbon Monoxide Poisoning)
Inflammatory myopathies (e.g., dermatomyositisDermatomyositisA subacute or chronic inflammatory disease of muscle and skin, marked by proximal muscle weakness and a characteristic skin rash. The illness occurs with approximately equal frequency in children and adults. The skin lesions usually take the form of a purplish rash (or less often an exfoliative dermatitis) involving the nose, cheeks, forehead, upper trunk, and arms. The disease is associated with a complement mediated intramuscular microangiopathy, leading to loss of capillaries, muscle ischemia, muscle-fiber necrosis, and perifascicular atrophy. The childhood form of this disease tends to evolve into a systemic vasculitis. Dermatomyositis may occur in association with malignant neoplasms.Paraneoplastic Syndromes)
Disturbance in myocyte calcium homeostasisMyocyte Calcium HomeostasisRhabdomyolysis (↑ in intracellular free ionized cytoplasmic and mitochondrial calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes) is the common cause of injury.
↑ Intracellular calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes leads to cell deathCell deathInjurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Apoptosis is programmed cell death, a mechanism with both physiologic and pathologic effects.Cell Injury and Death through:
Activation of enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes that produce cell injuryCell injuryThe cell undergoes a variety of changes in response to injury, which may or may not lead to cell death. Injurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Cell Injury and Death:
Endonucleases → deoxyribonucleic acidDeoxyribonucleic acidA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure (DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure) and chromatinChromatinThe material of chromosomes. It is a complex of dna; histones; and nonhistone proteins found within the nucleus of a cell.DNA Types and StructurefragmentationFragmentationChronic Apophyseal Injury
AdenosineAdenosineA nucleoside that is composed of adenine and d-ribose. Adenosine or adenosine derivatives play many important biological roles in addition to being components of DNA and RNA. Adenosine itself is a neurotransmitter.Class 5 Antiarrhythmic Drugs triphosphatases (ATPases) → adenosineAdenosineA nucleoside that is composed of adenine and d-ribose. Adenosine or adenosine derivatives play many important biological roles in addition to being components of DNA and RNA. Adenosine itself is a neurotransmitter.Class 5 Antiarrhythmic Drugs triphosphate(ATP) depletion
Production of reactive oxygen speciesReactive oxygen speciesMolecules or ions formed by the incomplete one-electron reduction of oxygen. These reactive oxygen intermediates include singlet oxygen; superoxides; peroxides; hydroxyl radical; and hypochlorous acid. They contribute to the microbicidal activity of phagocytes, regulation of signal transduction and gene expression, and the oxidative damage to nucleic acids; proteins; and lipids.Metabolic Dysfunction-associated Steatotic Liver Disease (MASLD) (ROS)
Additionally, ATP depletionATP depletionCell Injury and Death → dysfunction of the Na+/K+ ATPase and CaCACondylomata acuminata are a clinical manifestation of genital HPV infection. Condylomata acuminata are described as raised, pearly, flesh-colored, papular, cauliflower-like lesions seen in the anogenital region that may cause itching, pain, or bleeding.Condylomata Acuminata (Genital Warts)2+ ATPase pumps → loss of myocyte integrity → cell deathCell deathInjurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Apoptosis is programmed cell death, a mechanism with both physiologic and pathologic effects.Cell Injury and Death → release of intracellular components
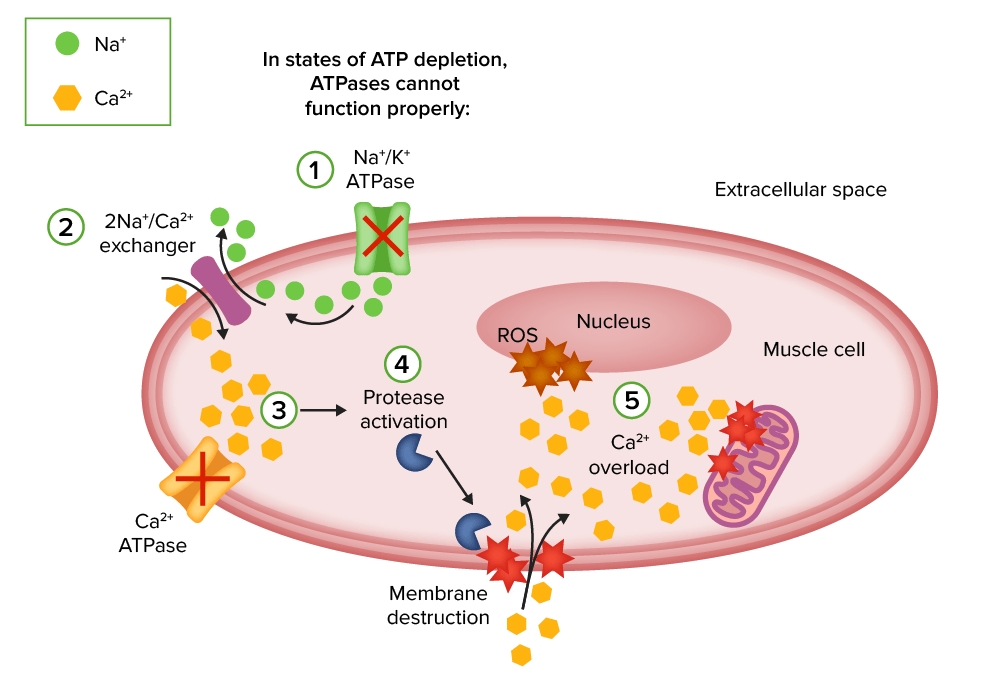
Injury mechanisms of rhabdomyolysis:
1. Energy (ATP) depletion inhibits Na+/K+ ATPase function and increases intracellular sodium.
2. The 2Na+/Ca2+ exchanger increases intracellular calcium.
3. Ca2+ ATPase is not able to pump out intracellular calcium due to energy depletion.
4. Intracellular calcium activates proteases such as phospholipase 2 (PLA2), which destroy the structural components of cell membranes and allow the entry of more calcium.
5. Calcium overload disrupts mitochondrial integrity and induces apoptosis, leading to necrosis of muscle cells.
ROS: reactive oxygen species
Image by Lecturio.
Renal injury[2,4]
Renal injury is the most common systemic complication of rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis. Factors contributing to renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome include:
Released enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes (including creatineCreatineAn amino acid that occurs in vertebrate tissues and in urine. In muscle tissue, creatine generally occurs as phosphocreatine. Creatine is excreted as creatinine in the urine.Acute Kidney Injury kinase (CK)) can damage capillariesCapillariesCapillaries are the primary structures in the circulatory system that allow the exchange of gas, nutrients, and other materials between the blood and the extracellular fluid (ECF). Capillaries are the smallest of the blood vessels. Because a capillary diameter is so small, only 1 RBC may pass through at a time.Capillaries: Histology
Subsequently, there is fluid leakage and sequestration in the extracellular spaces.
↓ Intravascular volume → stimulation of renin-angiotensin-aldosterone (RAA) system
RAA effect: reduced renal blood flowRenal blood flowThe amount of the renal blood flow that is going to the functional renal tissue, i.e., parts of the kidney that are involved in production of urine.Glomerular Filtration
Release of myoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis from necrotic muscles:
MyoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis is cytotoxicCytotoxicParvovirus B19 to nephrons.
MyoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis scavenges nitric oxideNitric OxideA free radical gas produced endogenously by a variety of mammalian cells, synthesized from arginine by nitric oxide synthase. Nitric oxide is one of the endothelium-dependent relaxing factors released by the vascular endothelium and mediates vasodilation. It also inhibits platelet aggregation, induces disaggregation of aggregated platelets, and inhibits platelet adhesion to the vascular endothelium. Nitric oxide activates cytosolic guanylate cyclase and thus elevates intracellular levels of cyclic gmp.Pulmonary Hypertension Drugs: ↑ renal injury
MyoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis also results in lipid peroxidationLipid peroxidationPeroxidase catalyzed oxidation of lipids using hydrogen peroxide as an electron acceptor.Drug-Induced Liver Injury of renal cell membranes.
Other components, including free ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements, can generate ROS and damage renal tubules.
Metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis: ↑ lactic acid from damaged/ischemic muscles
HyperphosphatemiaHyperphosphatemiaA condition of abnormally high level of phosphates in the blood, usually significantly above the normal range of 0. 84-1. 58 mmol per liter of serum.Hypocalcemia in necrotic muscles:
Leads to hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia
Leads to deposition of calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.ElectrolytesphosphatePhosphateInorganic salts of phosphoric acid.Electrolytes → renal damage
Uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis release:
NucleosidesNucleosidesPurine or pyrimidine bases attached to a ribose or deoxyribose.Nucleic Acids from cell nuclei → uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis
Deposition of uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis crystals increases in an acidic environment, leading to tubular obstruction.
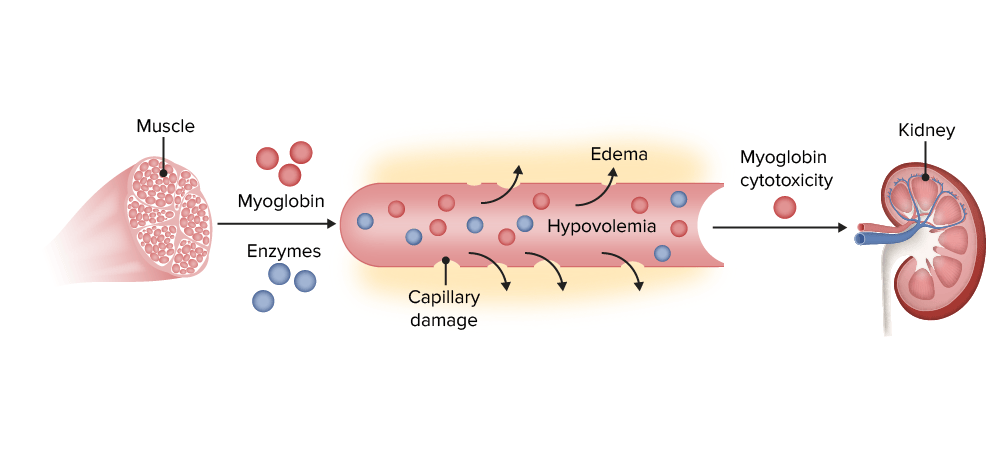
Acute kidney injury (AKI) in rhabdomyolysis (enzymes: creatine kinase, aldolase, lactate dehydrogenase):
After muscle destruction, myoglobin and enzymes are released into the circulation, damaging capillaries and leading to leakage and edema. Hypovolemia and reduced renal blood flow are associated with AKI. Myoglobin cytotoxicity affects the kidney due to lipid peroxidation and production of reactive oxygen species. Tubular obstruction by myoglobin is also associated with AKI.
< 10% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with the classic triad.
Children: Muscle painMuscle PainIon Channel Myopathy/tenderness, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, and viral prodromes are common symptoms.
Other patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with nonspecific symptoms (nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia).
Additional clues[2,4]
History:
Exertion (increased activity) or trauma
Immobility
Underlying conditions and medications
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
Findings that raise suspicion:
Dark urine without presenting genitourinary symptoms
Abnormal laboratory tests on presentation (electrolyte imbalance)
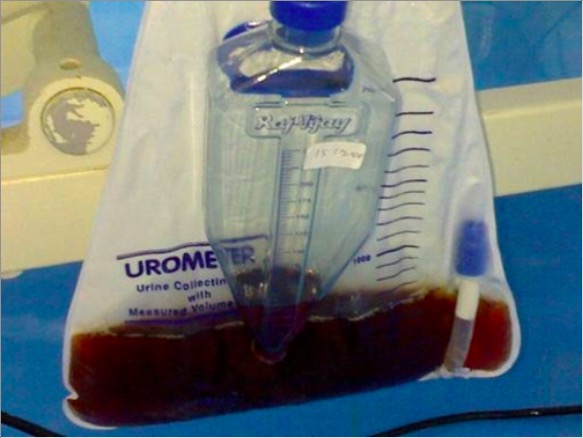
Tea-colored urine of a patient being treated for rhabdomyolysis
Image: “Urine appearance” by the Department of General Medicine, Sri Ramachandra University Chennai, Tamil Nadu, India. License: CC BY 3.0
Diagnosis
Laboratory abnormalities[2,4,5]
↑ CK (5 times the normal upper limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation or > 1,000 IU/L)
Key biomarker for rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis
Elevated at 12 hours after insult
Peaks at 24‒72 hours
Back to normal in about 5 days
↑ MyoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis:
May be hard to detect in serum (short half-lifeHalf-LifeThe time it takes for a substance (drug, radioactive nuclide, or other) to lose half of its pharmacologic, physiologic, or radiologic activity.Pharmacokinetics and Pharmacodynamics (1‒3 hours))
Serum level may be decreased before CK rises.
Causes red-to-brown urine
Detected by urinalysisUrinalysisExamination of urine by chemical, physical, or microscopic means. Routine urinalysis usually includes performing chemical screening tests, determining specific gravity, observing any unusual color or odor, screening for bacteriuria, and examining the sediment microscopically.Urinary Tract Infections (UTIs) in Children as myoglobinuriaMyoglobinuriaThe presence of myoglobin in urine usually as a result of rhabdomyolysis.Rhabdomyolysis: positive test for blood on the urine dipstick, but no RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology on microscopic examination
Electrolyte abnormalities (basic metabolic panelBasic Metabolic PanelPrimary vs Secondary Headaches, calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes, phosphorus):
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
HyperphosphatemiaHyperphosphatemiaA condition of abnormally high level of phosphates in the blood, usually significantly above the normal range of 0. 84-1. 58 mmol per liter of serum.Hypocalcemia
HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout: release of purinesPurinesA series of heterocyclic compounds that are variously substituted in nature and are known also as purine bases. They include adenine and guanine, constituents of nucleic acids, as well as many alkaloids such as caffeine and theophylline. Uric acid is the metabolic end product of purine metabolism.Nucleic Acids from the damaged muscle
HypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia: due to soft-tissue and muscle-cell damage → calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes enters myocytesMyocytesMature contractile cells, commonly known as myocytes, that form one of three kinds of muscle. The three types of muscle cells are skeletal, cardiac, and smooth. They are derived from embryonic (precursor) muscle cells called myoblasts.Muscle Tissue: Histology and calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes salts are deposited in the damaged muscle
Creatinine and BUN: for evidence of acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury (AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury)
Coagulation panel: for evidence of disseminated intravascular coagulationDisseminated intravascular coagulationDisseminated intravascular coagulation (DIC) is a condition characterized by systemic bodywide activation of the coagulation cascade. This cascade results in both widespread microvascular thrombi contributing to multiple organ dysfunction and consumption of clotting factors and platelets, leading to hemorrhage. Disseminated Intravascular Coagulation (DICDICDisseminated intravascular coagulation (DIC) is a condition characterized by systemic bodywide activation of the coagulation cascade. This cascade results in both widespread microvascular thrombi contributing to multiple organ dysfunction and consumption of clotting factors and platelets, leading to hemorrhage. Disseminated Intravascular Coagulation)
Arterial blood gasArterial blood gasRespiratory Alkalosis (ABG): for evidence of metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis
ElectrocardiographyElectrocardiographyRecording of the moment-to-moment electromotive forces of the heart as projected onto various sites on the body’s surface, delineated as a scalar function of time. The recording is monitored by a tracing on slow moving chart paper or by observing it on a cardioscope, which is a cathode ray tube display.Electrocardiogram (ECG) (ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG))[4]
To look for cardiac dysrhythmias (secondary to electrolyte abnormalities)
Possible findings of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia:
Ventricular tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
Possible finding with hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia: QTC prolongation
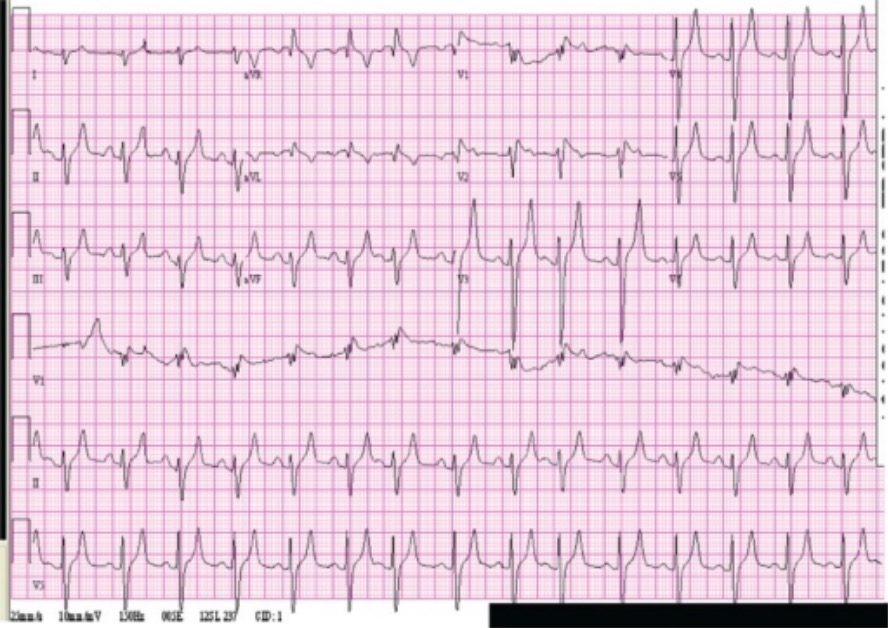
Patient with rhabdomyolysis and hyperkalemia: Electrocardiogram of a patient treated for rhabdomyolysis, showing peaked T waves and wide QRS. The patient had a serum potassium level of 8 mEq/L.
Image: “ Electrocardiogram” by Department of Medicine, Union Memorial Hospital, Baltimore, MD, USA. License: CC BY 2.0
Management
Local protocols may vary from location to location. The following information is based on current US and UK guidelines.
Initial approach[2,4]
AirwayAirwayABCDE Assessment, breathing, circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment (ABC) assessment for all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with trauma history
Exclude and treat other potential injuries (compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome, vascular compromise, fractures, dislocations, and wounds).
Removal of offending agents (if medication is suspected)
Correct/prevent hypoperfusion, lactic acidosisLactic AcidosisOxazolidinones, AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury
Treatment:
Lactated Ringer’sLactated Ringer’sA crystalloid solution that contains sodium chloride; sodium lactate; potassium chloride; and calcium chloride. It is used for fluid therapy.Fluid Replacement Therapy in Children or saline (0.9%‒0.45%)
Initial rate, 400 mL/hr; range, 400‒2,000 mL/hr
Titrate to urine output of 1‒3 mL/kg/hr up to a total of 300 mL/hr.
Caution for fluid overload in the anuric patient
Other therapies
BicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes therapy:
Limited clinical evidence to support the use of bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes therapy in the adult and pediatric populations with suspected rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis[5,6,8]
Some institutions may consider in severe cases:[2,7]
pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance < 7.3 or lactate > 4 (acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis)
No hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia
BicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes level < 30 mEq/L
Goal: urine pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance > 6.5 and serum pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance < 7.5
MannitolMannitolA diuretic and renal diagnostic aid related to sorbitol. It has little significant energy value as it is largely eliminated from the body before any metabolism can take place. It can be used to treat oliguria associated with kidney failure or other manifestations of inadequate renal function and has been used for determination of glomerular filtration rate. Mannitol is also commonly used as a research tool in cell biological studies, usually to control osmolarity.Osmotic Diuretics and loop diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication use is generally not supported by guidelines.[2,5,6]
Correction of electrolyte abnormalities[5,7]
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia(C BIG K drop):
Calcium chlorideChlorideInorganic compounds derived from hydrochloric acid that contain the Cl- ion.Electrolytes or gluconate (stabilizes cardiac myocytesMyocytesMature contractile cells, commonly known as myocytes, that form one of three kinds of muscle. The three types of muscle cells are skeletal, cardiac, and smooth. They are derived from embryonic (precursor) muscle cells called myoblasts.Muscle Tissue: Histology)
Beta-2 agonist (inhaled albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs)
Insulin infusion
Glucose infusion (D50 solution)
Kayexalate
HyperphosphatemiaHyperphosphatemiaA condition of abnormally high level of phosphates in the blood, usually significantly above the normal range of 0. 84-1. 58 mmol per liter of serum.Hypocalcemia:
Serum phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes increases because of release from damaged muscle cells.
Can bindBINDHyperbilirubinemia of the Newborn with serum calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes and deposit in tissue
Typically resolves spontaneously with urinary excretion
HypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia:
From entry into damaged muscle cells and bonding with phosphatePhosphateInorganic salts of phosphoric acid.Electrolytes/deposition in tissue
Avoid early treatment with calcium chlorideCalcium chlorideA salt used to replenish calcium levels, as an acid-producing diuretic, and as an antidote for magnesium poisoning.Hypocalcemia or gluconate, unless necessary for hyperkalemia-associated cardiac arrhythmias.
Usually resolves with appropriate fluid treatment
Rebound hypercalcemiaHypercalcemiaHypercalcemia (serum calcium > 10.5 mg/dL) can result from various conditions, the majority of which are due to hyperparathyroidism and malignancy. Other causes include disorders leading to vitamin D elevation, granulomatous diseases, and the use of certain pharmacological agents. Symptoms vary depending on calcium levels and the onset of hypercalcemia. Hypercalcemia is possible.
Monitoring[7]
CK levels every 6 hours until levels are consistently decreasing
Hourly urine output (urinary catheterization may be necessary)
ElectrocardiogramElectrocardiogramAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) and cardiac monitoring, if K+ is > 6.0 mEq/L
Renal replacement therapy (RRT)[2,5,7]
Not recommended for AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury prevention
Continuous or intermittent RRT may be needed for rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis with AKIAKIAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury that is refractory to medical management.
AnalgesiaAnalgesiaMethods of pain relief that may be used with or in place of analgesics.Anesthesiology: History and Basic Concepts (crush injuryCrush injuryExcessive compression of parts of the body that causes muscle swelling, fracture, and/or neurological disturbances in the affected areas. Crush injury with systemic manifestations is referred to as crush syndrome.Crush Syndrome)[7]
AcetaminophenAcetaminophenAcetaminophen is an over-the-counter nonopioid analgesic and antipyretic medication and the most commonly used analgesic worldwide. Despite the widespread use of acetaminophen, its mechanism of action is not entirely understood.Acetaminophen and limited opiatesOpiatesOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates.Opioid Analgesics
If painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, pallor, pulselessnessPulselessnessCardiac Arrest, paresthesia, poikilothermiaPoikilothermiaCold to the touch.Acute Limb Ischemia, and paralysis (the 6 PsPSInvasive Mechanical Ventilation) are present → emergency surgery consult needed for possible compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome
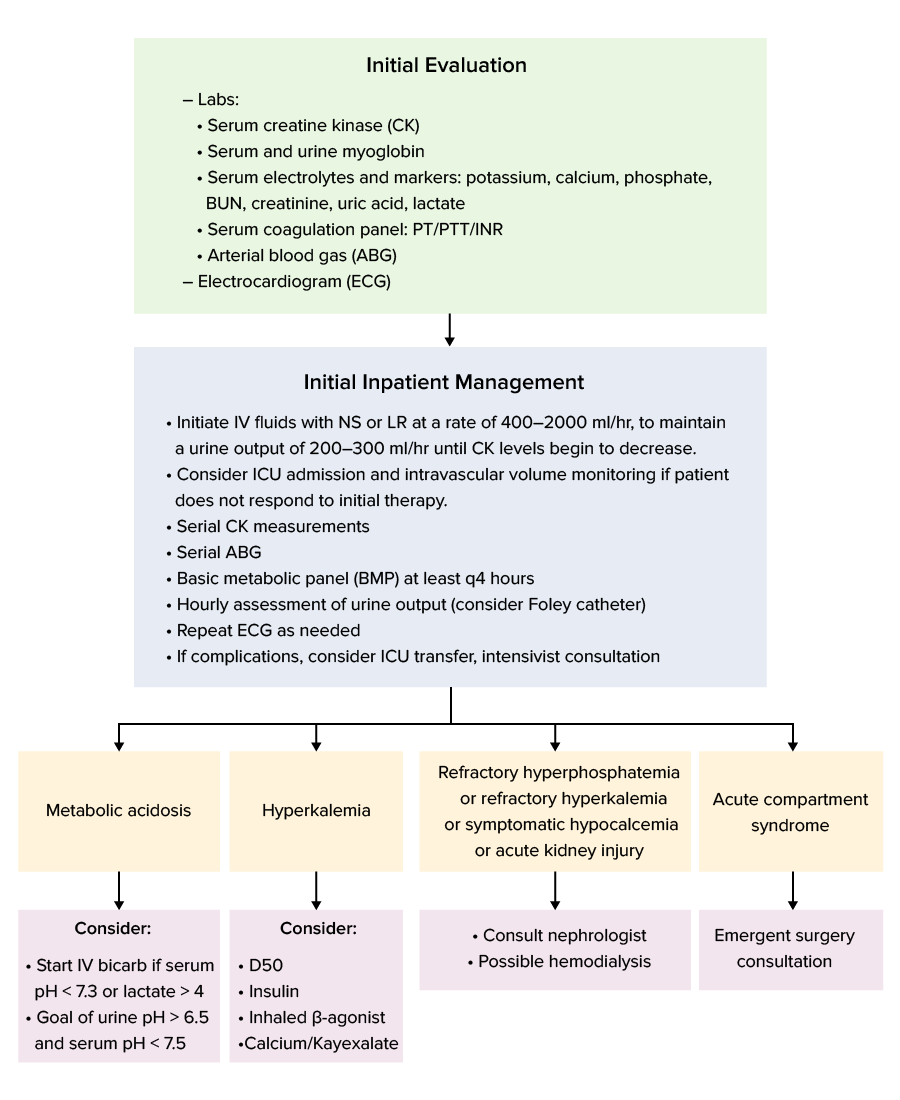
Management algorithm
Management algorithm for rhabdomyolysis
Image by Lecturio.
Clinical Relevance
ABC assessment: a mainstay management approach in managing critically ill patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship, which constitutes the 1st essential step in many situations, including unresponsive patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship, cardiac arrestCardiac arrestCardiac arrest is the sudden, complete cessation of cardiac output with hemodynamic collapse. Patients present as pulseless, unresponsive, and apneic. Rhythms associated with cardiac arrest are ventricular fibrillation/tachycardia, asystole, or pulseless electrical activity. Cardiac Arrest, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a history of trauma, or critically ill patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship. In patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with trauma, ABC is included in the primary surveyPrimary SurveyThoracic Trauma in Children, initial evaluation, and management of injuries.
Acute renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome: a sudden drop in the glomerular filtration rateGlomerular filtration rateThe volume of water filtered out of plasma through glomerular capillary walls into Bowman’s capsules per unit of time. It is considered to be equivalent to inulin clearance.Kidney Function Tests resulting from kidney damage, which occurs within a few hours to few days. Acute renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome is classified as prerenal, intrinsic, or postrenal, depending on the etiology. Management is based on causation and often revolves around aggressive fluid hydration. RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis results in acute tubular necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage from excessive filtered myoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis, leading to acute renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome.
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia: serum potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia (K+) level > 5.0 mEq/L. HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia results from several causes. Acute elevation in serum K+ (usually ≥ 7 mEq/L) can lead to cardiac arrhythmias and muscle weakness. Management involves myocardiumMyocardiumThe muscle tissue of the heart. It is composed of striated, involuntary muscle cells connected to form the contractile pump to generate blood flow.Heart: Anatomy stabilization, decreasing extracellular K+ levels, and enhancing K+ removal from the body.
HypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia: occurs when calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes levels are < 2.2 mmol/L or < 8.5 mg/dL. CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes levels are regulated by the parathyroidParathyroidThe parathyroid glands are 2 pairs of small endocrine glands found in close proximity to the thyroid gland. The superior parathyroid glands are lodged within the parenchyma of the upper poles of the right and left thyroid lobes; the inferior parathyroid glands are close to the inferior tips or poles of the lobes.Parathyroid Glands: Anatomy hormone (PTH). If the body fails to maintain normal calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes levels (especially ≤ 7.5 mg/dL), patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with arrhythmias, seizuresSeizuresA seizure is abnormal electrical activity of the neurons in the cerebral cortex that can manifest in numerous ways depending on the region of the brain affected. Seizures consist of a sudden imbalance that occurs between the excitatory and inhibitory signals in cortical neurons, creating a net excitation. The 2 major classes of seizures are focal and generalized. Seizures, and tetanyTetanyA disorder characterized by muscle twitches, cramps, and carpopedal spasm, and when severe, laryngospasm and seizures. This condition is associated with unstable depolarization of axonal membranes, primarily in the peripheral nervous system. Tetany usually results from hypocalcemia or reduced serum levels of magnesium that may be associated with hyperventilation; hypoparathyroidism; rickets; uremia; or other conditions.Hypocalcemia. Management is by calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes replacement.
HyperuricemiaHyperuricemiaExcessive uric acid or urate in blood as defined by its solubility in plasma at 37 degrees c; greater than 0. 42 mmol per liter (7. 0 mg/dl) in men or 0. 36 mmol per liter (6. 0 mg/dl) in women.Gout: elevated uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis levels resulting from accelerated purine degradation (observed in high cell-turnover states, including rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis). Large uric acidUric acidAn oxidation product, via xanthine oxidase, of oxypurines such as xanthine and hypoxanthine. It is the final oxidation product of purine catabolism in humans and primates, whereas in most other mammals urate oxidase further oxidizes it to allantoin.Nephrolithiasis deposits in renal tubules cause acute renal injury. Management involves aggressive intravenous hydration.
Compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome: a surgical emergencySurgical EmergencyAcute Abdomen occurring secondary to trauma. Compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome is marked by increased pressure within a compartment, compromising circulationCirculationThe movement of the blood as it is pumped through the cardiovascular system.ABCDE Assessment and tissue function. Long-bone fractures are the most common cause. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, pallor, pulselessnessPulselessnessCardiac Arrest, paresthesia, poikilothermiaPoikilothermiaCold to the touch.Acute Limb Ischemia, and paralysis (the 6 PsPSInvasive Mechanical Ventilation). Diagnosis is clinical, but compartment-pressure measurement can be used. Management is by emergency fasciotomyFasciotomySurgical incision on the fascia. It is used to decompress compartment pressure (e.g. in compartment syndromes; circumferential burns and extremity injuries) or to release contractures (e.g. in dupuytren’s contracture).Compartment Syndrome.
Crush syndromeCrush SyndromeCrush syndrome encompasses the systemic manifestations that result from a crush (or traumatic compression) injury. Compartment syndrome and/or rhabdomyolysis can also occur in crush syndrome. Systemic effects include the development of renal failure due to toxins released from damaged muscles, hypovolemia, and acidosis. Crush Syndrome: systemic manifestations (renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome, shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock) resulting from compressive traumatic injury. Compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome and/or rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis can occur in Crush syndromeCrush SyndromeCrush syndrome encompasses the systemic manifestations that result from a crush (or traumatic compression) injury. Compartment syndrome and/or rhabdomyolysis can also occur in crush syndrome. Systemic effects include the development of renal failure due to toxins released from damaged muscles, hypovolemia, and acidosis. Crush Syndrome. Field management with intravenous fluidsIntravenous FluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids and extrication is crucial in reducing the risk of complications and death.
HeatstrokeHeatstrokeHeatstroke is an illness characterized as a core body temperature exceeding 40°C (104°F) with accompanying neurological symptoms including ataxia, seizures, and/or delirium. Heatstroke is usually due to the body’s inability to regulate its temperature when challenged with an elevated heat load. Heatstroke: a condition associated with hyperthermia (elevation of core body temperatureBody TemperatureThe measure of the level of heat of a human or animal.Heatstroke above the normal diurnal range of 36ºC–37.5ºC (96.8ºF–99.5ºF) owing to failure in thermoregulationThermoregulationBody temperature can be divided into external temperature, which involves the skin, and core temperature, which involves the CNS and viscera. While external temperature can be variable, the core temperature is maintained within a narrow range of 36.5-37.5ºC (97.7-99.5ºF).Body Temperature Regulation). HeatstrokeHeatstrokeHeatstroke is an illness characterized as a core body temperature exceeding 40°C (104°F) with accompanying neurological symptoms including ataxia, seizures, and/or delirium. Heatstroke is usually due to the body’s inability to regulate its temperature when challenged with an elevated heat load. Heatstroke is either exertional or non-exertional and can be complicated by rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis. Cooling measures with fluid and electrolyte replacement are recommended.
Billing and Coding
Diagnosis Codes:
This code is used to formally document rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis, a condition involving rapid breakdown of skeletal muscle tissue, which releases damaging proteinsProteinsLinear polypeptides that are synthesized on ribosomes and may be further modified, crosslinked, cleaved, or assembled into complex proteins with several subunits. The specific sequence of amino acids determines the shape the polypeptide will take, during protein folding, and the function of the protein.Energy Homeostasis into the blood.
Coding System
Code
Description
ICD-10-CM
M62.82
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis
SNOMED CT
241696005
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis (disorder)
Evaluation & Workup:
This CPT code is for measuring the creatineCreatineAn amino acid that occurs in vertebrate tissues and in urine. In muscle tissue, creatine generally occurs as phosphocreatine. Creatine is excreted as creatinine in the urine.Acute Kidney Injury kinase (CK) level, the key laboratory test for diagnosing and monitoring rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis, as levels are typically dramatically elevated.
Coding System
Code
Description
CPT
82550
CreatineCreatineAn amino acid that occurs in vertebrate tissues and in urine. In muscle tissue, creatine generally occurs as phosphocreatine. Creatine is excreted as creatinine in the urine.Acute Kidney Injury kinase (CK), (CPK); total
CPT
80053
Comprehensive metabolic panelComprehensive metabolic panelPrimary vs Secondary Headaches (to check potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia and kidney function)
Procedures/Interventions:
The cornerstone of treatment is aggressive intravenous fluid hydration to flush the kidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy and prevent damage. DialysisDialysisRenal replacement therapy refers to dialysis and/or kidney transplantation. Dialysis is a procedure by which toxins and excess water are removed from the circulation. Hemodialysis and peritoneal dialysis (PD) are the two types of dialysis, and their primary difference is the location of the filtration process (external to the body in hemodialysis versus inside the body for PD).Peritoneal Dialysis and Hemodialysis may be required if acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury becomes severe.
Coding System
Code
Description
CPT
96360
Intravenous infusion, hydration; initial, 31 minutes to 1 hour
CPT
90935
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome procedure
Complications:
These codes document the most serious complications of rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis: acute kidney injuryAcute Kidney InjuryAcute kidney injury refers to sudden and often reversible loss of renal function, which develops over days or weeks. Azotemia refers to elevated levels of nitrogen-containing substances in the blood that accompany AKI, which include BUN and creatinine. Acute Kidney Injury from myoglobinMyoglobinA conjugated protein which is the oxygen-transporting pigment of muscle. It is made up of one globin polypeptide chain and one heme group.Rhabdomyolysis clogging the renal tubules, and life-threatening hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia from potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia release from damaged muscle cells.
Coding System
Code
Description
ICD-10-CM
N17.9
Acute kidney failure, unspecified
ICD-10-CM
E87.5
HyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia
References
Beck M. A., Haller P. (2020). Compartment syndrome. In Tintinalli, J. E., Ma, O., Yealy, D. M., Meckler, G. D., Stapczynski, J., Cline, D. M., Thomas, S. H. (Eds.), Tintinalli’s Emergency Medicine: A Comprehensive Study Guide (9th ed.). McGraw-Hill.
Chavez, L. O., Leon, M., Einav, S., Varon, J. (2016). Beyond muscle destruction: a systematic review of rhabdomyolysis for clinical practice. Critical Care, 20(1), 135. https://doi.org/10.1186/s13054-016-1314-5
Kodadek, L., Carmichael, S. P., II, Seshadri, A., Pathak, A., Hoth, J., Appelbaum, R., Michetti, C. P., Gonzalez, R. P. (2022). Rhabdomyolysis: an American Association for the Surgery of Trauma Critical Care Committee clinical consensus document. Trauma Surgery & Acute Care Open, 7(1), e000836. https://doi.org/10.1136/tsaco-2021-000836
Nye, N. S., Kasper, K., Madsen, C. M., Szczepanik, M., Covey, C. J., Oh, R., Kane, S., Beutler, A. I., Leggit, J. C., Deuster, P. A., O’Connor, F. G. (2021). Clinical practice guidelines for exertional rhabdomyolysis: a military medicine perspective. Current Sports Medicine Reports, 20(3), 169–178. https://doi.org/10.1249/JSR.0000000000000822