Reactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The pathophysiology of this disease is unclear, but a significant proportion of affected patients are positive for HLA-B27. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis. Ocular, mucocutaneous, GI, GU, and cardiac manifestations may also occur. The diagnosis is clinical, and efforts should be made to rule out alternative diagnoses. Management focuses on controlling symptoms, typically with nonsteroidal anti-inflammatory drugs. An active infection, particularly Chlamydia trachomatis, should also be treated.
Reactive arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis (ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis) is an autoimmune, post-infectious, seronegative spondyloarthritis.
ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis develops in:
1%–3% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with urethritisUrethritisInflammation involving the urethra. Similar to cystitis, clinical symptoms range from vague discomfort to painful urination (dysuria), urethral discharge, or both.Urinary Tract Infections (UTIs)
1%–4% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with an enteric infection
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 0.6–27 cases per 100,000 worldwide
PrevalencePrevalenceThe total number of cases of a given disease in a specified population at a designated time. It is differentiated from incidence, which refers to the number of new cases in the population at a given time.Measures of Disease Frequency: 30–40 per 100,000 adults
More common in men
Occurs more frequently in young adults (< 40 years of age)
70%–90% have the HLA-B27 alleleAlleleVariant forms of the same gene, occupying the same locus on homologous chromosomes, and governing the variants in production of the same gene product.Basic Terms of Genetics
Etiology[1–4,13–15,17]
Generally occurs 1–4 weeks after certain infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease:
Genitourinary (GU):
Chlamydia trachomatisChlamydia trachomatisType species of Chlamydia causing a variety of ocular and urogenital diseases.Chlamydia(most common)
Neisseria gonorrhoeaeNeisseria gonorrhoeaeA species of gram-negative, aerobic bacteria primarily found in purulent venereal discharges. It is the causative agent of gonorrhea.Neisseria
Ureaplasma urealyticum
Gastrointestinal (GI):
Campylobacter jejuniCampylobacter jejuniA species of bacteria that resemble small tightly coiled spirals. Its organisms are known to cause abortion in sheep and fever and enteritis in man and may be associated with enteric diseases of calves, lambs, and other animals.Campylobacter(most common)
Shigella flexneriShigella flexneriA bacterium which is one of the etiologic agents of bacillary dysentery and sometimes of infantile gastroenteritis.Shigella, S. dysenteriaeS. dysenteriaeA species of gram-negative, facultatively anaerobic, rod-shaped bacteria that is extremely pathogenic and causes severe dysentery. Infection with this organism often leads to ulceration of the intestinal epithelium.Shigella, andS. sonneiS. sonneiA lactose-fermenting bacterium causing dysentery.Shigella
Salmonella entericaSalmonella entericaA subgenus of Salmonella containing several medically important serotypes. The habitat for the majority of strains is warm-blooded animals.Salmonella
Escherichia coliEscherichia coliThe gram-negative bacterium Escherichia coli is a key component of the human gut microbiota. Most strains of E. coli are avirulent, but occasionally they escape the GI tract, infecting the urinary tract and other sites. Less common strains of E. coli are able to cause disease within the GI tract, most commonly presenting as abdominal pain and diarrhea. Escherichia coli
Pulmonary (less common):
ChlamydiaChlamydiaChlamydiae are obligate intracellular gram-negative bacteria. They lack a peptidoglycan layer and are best visualized using Giemsa stain. The family of Chlamydiaceae comprises 3 pathogens that can infect humans: Chlamydia trachomatis, Chlamydia psittaci, and Chlamydia pneumoniae.ChlamydiapneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia
Mycobacterium tuberculosisMycobacterium tuberculosisTuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis complex bacteria. The bacteria usually attack the lungs but can also damage other parts of the body. Approximately 30% of people around the world are infected with this pathogen, with the majority harboring a latent infection. Tuberculosis spreads through the air when a person with active pulmonary infection coughs or sneezes.Tuberculosis
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation at the site of ligament, tendon, fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis, or joint capsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.Bacteroides insertion to boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types
Plantar fasciaPlantar fasciaFoot: Anatomy insertion site on the calcaneusCalcaneusThe largest of the tarsal bones which is situated at the lower and back part of the foot, forming the heel.Foot: Anatomy
Ischial tuberosities
Iliac crests
Tibial tuberosities
RibsRibsA set of twelve curved bones which connect to the vertebral column posteriorly, and terminate anteriorly as costal cartilage. Together, they form a protective cage around the internal thoracic organs.Chest Wall: Anatomy
TendonitisTendonitisReactive Arthritis and periostitisPeriostitisInflammation of the periosteum. The condition is generally chronic, and is marked by tenderness and swelling of the bone and an aching pain. Acute periostitis is due to infection, is characterized by diffuse suppuration, severe pain, and constitutional symptoms, and usually results in necrosis.Reactive Arthritis:[2–4,12,15]
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the tendon or periosteumPeriosteumThin outer membrane that surrounds a bone. It contains connective tissue, capillaries, nerves, and a number of cell types.Bones: Structure and Types, respectively
Plantar fasciitisPlantar fasciitisInflammation of the plantar fascia (aponeurosis) on the bottom of the foot causing heel pain. The etiology of plantar fasciitis remains controversial but is likely to involve a biomechanical imbalance. Though often presenting along with heel spur, they do not appear to be causally related.Ankle and Foot Pain
Digital periostitisPeriostitisInflammation of the periosteum. The condition is generally chronic, and is marked by tenderness and swelling of the bone and an aching pain. Acute periostitis is due to infection, is characterized by diffuse suppuration, severe pain, and constitutional symptoms, and usually results in necrosis.Reactive Arthritis
SacroiliitisSacroiliitisInflammation of the sacroiliac joint. It is characterized by lower back pain, especially upon walking, fever, uveitis; psoriasis; and decreased range of motion. Many factors are associated with and cause sacroiliitis including infection; injury to spine, lower back, and pelvis; degenerative arthritis; and pregnancy.Ankylosing Spondylitis:[2,3,12,15]
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the sacroiliac joints
Signs and symptoms:
Low back painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
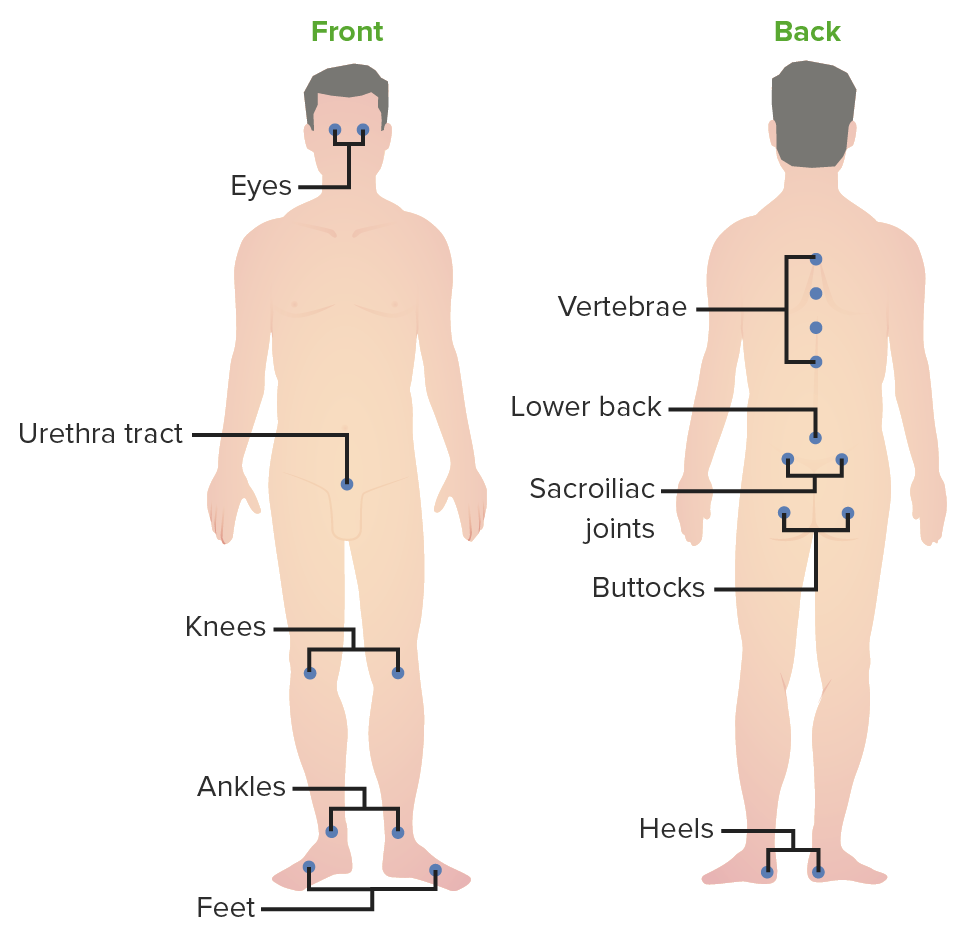
Common inflammatory sites in ReA: Image demonstrates the common joints involved in ReA. Conjunctivitis and urethritis are also frequent manifestations, and are part of the clinical triad for ReA.
Image by Lecturio.
Extra-articular manifestations
Ocular:[1–4,11–13,15]
ConjunctivitisConjunctivitisConjunctivitis is a common inflammation of the bulbar and/or palpebral conjunctiva. It can be classified into infectious (mostly viral) and noninfectious conjunctivitis, which includes allergic causes. Patients commonly present with red eyes, increased tearing, burning, foreign body sensation, and photophobia. Conjunctivitis
Anterior uveitisUveitisUveitis is the inflammation of the uvea, the pigmented middle layer of the eye, which comprises the iris, ciliary body, and choroid. The condition is categorized based on the site of disease; anterior uveitis is the most common. Diseases of the Uvea
UrethritisUrethritisInflammation involving the urethra. Similar to cystitis, clinical symptoms range from vague discomfort to painful urination (dysuria), urethral discharge, or both.Urinary Tract Infections (UTIs)
ProstatitisProstatitisProstatitis is inflammation or an irritative condition of the prostate that presents as different syndromes: acute bacterial, chronic bacterial, chronic prostatitis/chronic pelvic pain, and asymptomatic. Bacterial prostatitis is easier to identify clinically and the management (antibiotics) is better established. Prostatitis
CystitisCystitisInflammation of the urinary bladder, either from bacterial or non-bacterial causes. Cystitis is usually associated with painful urination (dysuria), increased frequency, urgency, and suprapubic pain.Urinary Tract Infections (UTIs)
Painless oral ulcersOral ulcersA loss of mucous substance of the mouth showing local excavation of the surface, resulting from the sloughing of inflammatory necrotic tissue. It is the result of a variety of causes, e.g., denture irritation, aphthous stomatitis; necrotizing gingivitis, toothbrushing, and various irritants.Chédiak-Higashi Syndrome
Nail dystrophy
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion nodosum (uncommon)
GI:[1–4,12]
Intermittent diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
ColitisColitisInflammation of the colon section of the large intestine, usually with symptoms such as diarrhea (often with blood and mucus), abdominal pain, and fever.Pseudomembranous Colitis
Presentation of acute viral conjunctivitis: Conjunctivitis, which is typically seen with viral infection of the pharynx
Image: “Acute viral conjunctivitis” by Wikimedia Creative Commons. License: CC BY 4.0
Keratoderma blennorrhagicum:
A cutaneous manifestation of reactive arthritis, which commonly affects the palms and soles
Image: “File:Feet-Reiters syndrome” by CDC/ Dr. M. F. Rein. License: Public Domain
Balanitis circinata:
Another possible extra-articular manifestation of reactive arthritis.
Image: “Penis with Balanitis Circinata, a rheumatic disease with nearly identical symptoms to mycosis infection” by Freakedenough. License: CC BY-SA 4.0
Clinical triad[11,15]
This classic triad of symptoms is found in only about 30% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis:
ConjunctivitisConjunctivitisConjunctivitis is a common inflammation of the bulbar and/or palpebral conjunctiva. It can be classified into infectious (mostly viral) and noninfectious conjunctivitis, which includes allergic causes. Patients commonly present with red eyes, increased tearing, burning, foreign body sensation, and photophobia. Conjunctivitis
UrethritisUrethritisInflammation involving the urethra. Similar to cystitis, clinical symptoms range from vague discomfort to painful urination (dysuria), urethral discharge, or both.Urinary Tract Infections (UTIs)
Mnemonic: “Can’t see, can’t pee, and can’t climb a tree.”
Diagnosis
Reactive arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis is a clinical diagnosis based on: [5,6,13,15,17]
Performed in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with joint effusions
Findings are nonspecific.
↑ LeukocytesLeukocytesWhite blood cells. These include granular leukocytes (basophils; eosinophils; and neutrophils) as well as non-granular leukocytes (lymphocytes and monocytes).White Myeloid Cells: Histology with neutrophil predominance may be seen (5,000‒50,000 WBCs per high-power field (HPF))[10]
Mild leukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus on complete blood cell count (CBC)
Stool PCRStool PCRNorovirus and/or cultures → evaluate for causative organisms if the patient has diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Urine or genital swab → evaluate for C. trachomatis
Urine cultureUrine cultureUrinary Tract Infections (UTIs) → Ureaplasma or ChlamydiaChlamydiaChlamydiae are obligate intracellular gram-negative bacteria. They lack a peptidoglycan layer and are best visualized using Giemsa stain. The family of Chlamydiaceae comprises 3 pathogens that can infect humans: Chlamydia trachomatis, Chlamydia psittaci, and Chlamydia pneumoniae.Chlamydia
HLA-B27 testing → supports the diagnosis in conjunction with the clinical picture
HIVHIVAnti-HIV Drugs and tuberculinTuberculinA protein extracted from boiled culture of tubercle bacilli (Mycobacterium tuberculosis). It is used in the tuberculin skin test (tuberculin test) for the diagnosis of tuberculosis infection in asymptomatic persons.Type IV Hypersensitivity ReactionskinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions testing in high-risk individuals (high association with ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis)
Rheumatoid factorRheumatoid factorAntibodies found in adult rheumatoid arthritis patients that are directed against gamma-chain immunoglobulins.Autoimmune Hepatitis (RFRFRheumatoid Arthritis) and anti–cyclic citrullinated peptide (anti-CCP) → rule out rheumatoid arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis
Radiographs of affected joints:[5,6,13,17]
Findings are generally nonspecific.
Can be used to evaluate for evidence of:
Fractures
Ankylosing spondylitisAnkylosing spondylitisAnkylosing spondylitis (also known as Bechterew’s disease or Marie-Strümpell disease) is a seronegative spondyloarthropathy characterized by chronic and indolent inflammation of the axial skeleton. Severe disease can lead to fusion and rigidity of the spine. Ankylosing Spondylitis in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with sacroiliitisSacroiliitisInflammation of the sacroiliac joint. It is characterized by lower back pain, especially upon walking, fever, uveitis; psoriasis; and decreased range of motion. Many factors are associated with and cause sacroiliitis including infection; injury to spine, lower back, and pelvis; degenerative arthritis; and pregnancy.Ankylosing Spondylitis
May show:
Joint space narrowing
Soft tissueSoft TissueSoft Tissue AbscessedemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Periosteal new boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types formation
Management may vary depending on practice location. The following information is based on US, UK, and European literature.
Treatment of ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis is supportive. Symptoms of ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis typically resolve in 3‒4 months, but prolonged or recurrent symptoms can occur in up to 50% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
NaproxenNaproxenAn anti-inflammatory agent with analgesic and antipyretic properties. Both the acid and its sodium salt are used in the treatment of rheumatoid arthritis and other rheumatic or musculoskeletal disorders, dysmenorrhea, and acute gout.Nonsteroidal Antiinflammatory Drugs (NSAIDs) 500 mg orally 2‒3 times/day; maximum 1,250 mg/day
IbuprofenIbuprofenA nonsteroidal anti-inflammatory agent with analgesic properties used in the treatment of rheumatism and arthritis.Nonsteroidal Antiinflammatory Drugs (NSAIDs) 300‒400 mg orally 3‒4 times/day; maximum 2,400 mg/day
DiclofenacDiclofenacA non-steroidal anti-inflammatory agent (nsaid) with antipyretic and analgesic actions. It is primarily available as the sodium salt.Nonsteroidal Antiinflammatory Drugs (NSAIDs) 50 mg orally 3 times/day
IndomethacinIndomethacinA non-steroidal anti-inflammatory agent (nsaid) that inhibits cyclooxygenase, which is necessary for the formation of prostaglandins and other autacoids. It also inhibits the motility of polymorphonuclear leukocytes.Nonsteroidal Antiinflammatory Drugs (NSAIDs) 50 mg orally 3 times/day
Try 2 different classes for 3‒4 weeks, then proceed to alternative treatment
Intra-articular glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids:[5‒7,13,16,17]
TriamcinoloneTriamcinoloneA glucocorticoid given, as the free alcohol or in esterified form, orally, intramuscularly, by local injection, by inhalation, or applied topically in the management of various disorders in which corticosteroids are indicated.Glucocorticoids acetonide 10‒40 mg in affected joint(s)
MethylprednisoloneMethylprednisoloneA prednisolone derivative with similar anti-inflammatory action.Immunosuppressants acetate 40‒80 mg in affected joint(s)
May repeat after 3 months if adequate painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief after 1st injection and symptoms have returned
2nd-line therapy:[5–7,13,15,17]
Indicated if the above treatments fail
Systemic corticosteroidsCorticosteroidsChorioretinitis (prednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants/prednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants): 0.5‒1 mg/kg/day orally, gradual taper, as soon as possible
Disease-modifying antirheumatic drugsDisease-modifying antirheumatic drugsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs) (DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs)):
SulfasalazineSulfasalazineA drug that is used in the management of inflammatory bowel diseases. Its activity is generally considered to lie in its metabolic breakdown product, 5-aminosalicylic acid released in the colon.Sulfonamides and Trimethoprim 500 mg by mouth once daily; may increase by 500 mg/day on a weekly basis; maximum, 2‒3 g/day divided into 2‒3 doses
MethotrexateMethotrexateAn antineoplastic antimetabolite with immunosuppressant properties. It is an inhibitor of tetrahydrofolate dehydrogenase and prevents the formation of tetrahydrofolate, necessary for synthesis of thymidylate, an essential component of DNA.Antimetabolite Chemotherapy (psoriatic/rheumatoid arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis dosing): 15‒25 mg by mouth, once a week
DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs)
SulfasalazineSulfasalazineA drug that is used in the management of inflammatory bowel diseases. Its activity is generally considered to lie in its metabolic breakdown product, 5-aminosalicylic acid released in the colon.Sulfonamides and Trimethoprim
MethotrexateMethotrexateAn antineoplastic antimetabolite with immunosuppressant properties. It is an inhibitor of tetrahydrofolate dehydrogenase and prevents the formation of tetrahydrofolate, necessary for synthesis of thymidylate, an essential component of DNA.Antimetabolite Chemotherapy
TumorTumorInflammationnecrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage factor (TNFTNFTumor necrosis factor (TNF) is a major cytokine, released primarily by macrophages in response to stimuli. The presence of microbial products and dead cells and injury are among the stimulating factors. This protein belongs to the TNF superfamily, a group of ligands and receptors performing functions in inflammatory response, morphogenesis, and cell proliferation. Tumor Necrosis Factor (TNF)) inhibitors
Considered in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who do not respond to DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs)
Limited data
Examples of agents used:
AdalimumabAdalimumabA humanized monoclonal antibody that binds specifically to tnf-alpha and blocks its interaction with endogenous tnf receptors to modulate inflammation. It is used in the treatment of rheumatoid arthritis; psoriatic arthritis; Crohn’s disease and ulcerative colitis.Disease-Modifying Antirheumatic Drugs (DMARDs)
EtanerceptEtanerceptA recombinant version of soluble human tnf receptor fused to an IgG Fc fragment that binds specifically to tumor necrosis factor and inhibits its binding with endogenous tnf receptors. It prevents the inflammatory effect of tnf and is used to treat rheumatoid arthritis; psoriatic arthritis and ankylosing spondylitis.Immunosuppressants
DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs):
SulfasalazineSulfasalazineA drug that is used in the management of inflammatory bowel diseases. Its activity is generally considered to lie in its metabolic breakdown product, 5-aminosalicylic acid released in the colon.Sulfonamides and Trimethoprim
MethotrexateMethotrexateAn antineoplastic antimetabolite with immunosuppressant properties. It is an inhibitor of tetrahydrofolate dehydrogenase and prevents the formation of tetrahydrofolate, necessary for synthesis of thymidylate, an essential component of DNA.Antimetabolite Chemotherapy
Consider a 12-week course before advancing to tumorTumorInflammationnecrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage factor (TNFTNFTumor necrosis factor (TNF) is a major cytokine, released primarily by macrophages in response to stimuli. The presence of microbial products and dead cells and injury are among the stimulating factors. This protein belongs to the TNF superfamily, a group of ligands and receptors performing functions in inflammatory response, morphogenesis, and cell proliferation. Tumor Necrosis Factor (TNF)) inhibitors.
Considered in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who do not respond to DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs)
Limited data
Management of extra-articular manifestations
Ocular:[5,6,11,15]
Referral for ophthalmologic evaluation
Anterior uveitisUveitisUveitis is the inflammation of the uvea, the pigmented middle layer of the eye, which comprises the iris, ciliary body, and choroid. The condition is categorized based on the site of disease; anterior uveitis is the most common. Diseases of the Uvea: corticosteroid and mydriatic eye drops
ConjunctivitisConjunctivitisConjunctivitis is a common inflammation of the bulbar and/or palpebral conjunctiva. It can be classified into infectious (mostly viral) and noninfectious conjunctivitis, which includes allergic causes. Patients commonly present with red eyes, increased tearing, burning, foreign body sensation, and photophobia. Conjunctivitis: symptomatic treatment
Mucocutaneous:[5,6,15,17]
Symptomatic treatment for mild lesions
Topical steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors
Topical salicylates
Vitamin DVitamin DA vitamin that includes both cholecalciferols and ergocalciferols, which have the common effect of preventing or curing rickets in animals. It can also be viewed as a hormone since it can be formed in skin by action of ultraviolet rays upon the precursors, 7-dehydrocholesterol and ergosterol, and acts on vitamin D receptors to regulate calcium in opposition to parathyroid hormone.Fat-soluble Vitamins and their Deficiencies analogs
Severe keratoderma blennorrhagica:
Topical steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors
DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs)
BalanitisBalanitisInflammation of the head of the penis, glans penis.Penile Anomalies and Conditions circinata: genital hygiene and topical steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors
Management of underlying infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
ImmunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.GastroenteritispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
GU infection:
C. trachomatis treatment:[8,15,16]
Doxycycline 100 mg by mouth twice daily for 7 days (recommended)
Alternatives:
AzithromycinAzithromycinA semi-synthetic macrolide antibiotic structurally related to erythromycin. It has been used in the treatment of Mycobacterium avium intracellulare infections, toxoplasmosis, and cryptosporidiosis.Macrolides and Ketolides (used in pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care) 1 g by mouth for 1 dose
N.gonorrhoeae: ceftriaxoneCeftriaxoneA broad-spectrum cephalosporin antibiotic and cefotaxime derivative with a very long half-life and high penetrability to meninges, eyes and inner ears.Cephalosporins:[9,15,16]
< 150 kg: 500 mg IM in a single dose
≥ 150 kg: 1 g IM in a single dose
Note about infection treatment: antibiotic therapy aims to eradicate the underlying infection but does not alter the progression of arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis in most cases.
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas[4,10–13,17]
Most cases resolve within 6 months.
Factors associated with more severe or persistent disease):
Male sexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender Dysphoria
Gonococcal arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis: an infection due direct bacterial invasion of N.gonorrhoeae. Disseminated disease can present similar to ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis with an acute, inflammatory, asymmetric arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis with urethritisUrethritisInflammation involving the urethra. Similar to cystitis, clinical symptoms range from vague discomfort to painful urination (dysuria), urethral discharge, or both.Urinary Tract Infections (UTIs). Diagnosis is based on the clinical history, synovial fluid analysisSynovial Fluid AnalysisRheumatoid Arthritis, and culture results. Management includes antibiotics.
Behcet’s disease: an inflammatory vasculitisVasculitisInflammation of any one of the blood vessels, including the arteries; veins; and rest of the vasculature system in the body.Systemic Lupus Erythematosus of small and large vessels. Symptoms can include arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis and painful oral and genital ulcers, unlike the painless lesions in ReAReAReactive arthritis is a seronegative autoimmune spondyloarthropathy that occurs in response to a previous gastrointestinal (GI) or genitourinary (GU) infection. The disease manifests as asymmetric oligoarthritis (particularly of large joints in the lower extremities), enthesopathy, dactylitis, and/or sacroiliitis.Reactive Arthritis. Ocular, neurologic, GI, and vascular manifestations are also seen. Diagnosis is based on clinical criteria. Management depends on the clinical manifestations and includes corticosteroidsCorticosteroidsChorioretinitis, DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs), and TNF inhibitorsTNF inhibitorsAnkylosing Spondylitis.
Rheumatoid arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis: an autoimmune disease resulting in joint inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation and destruction. This arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis is typically symmetric, and patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will frequently have tender inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation in the joints of the hands and feet (although any peripheral joints can be involved). The axialAxialComputed Tomography (CT) skeleton is less commonly included. Diagnosis is made with positive RFRFRheumatoid Arthritis and anti-CCP laboratory studies. Management includes NSAIDsNSAIDSPrimary vs Secondary Headaches, DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs), corticosteroidsCorticosteroidsChorioretinitis, immunosuppressive medications, biologics, and TNF inhibitorsTNF inhibitorsAnkylosing Spondylitis.
Psoriatic arthritisPsoriatic ArthritisA type of inflammatory arthritis associated with psoriasis, often involving the axial joints and the peripheral terminal interphalangeal joints. It is characterized by the presence of hla-b27-associated spondyloarthropathy, and the absence of rheumatoid factor.Psoriasis: a spondyloarthropathySpondyloarthropathyAnkylosing Spondylitis that occurs in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with psoriasisPsoriasisPsoriasis is a common T-cell-mediated inflammatory skin condition. The etiology is unknown, but is thought to be due to genetic inheritance and environmental triggers. There are 4 major subtypes, with the most common form being chronic plaque psoriasis. Psoriasis. This inflammatory arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis is frequently asymmetric. The small and large joints are involved, including the distal interphalangeal jointsInterphalangeal jointsHand: Anatomy and the sacroiliac spineSpineThe human spine, or vertebral column, is the most important anatomical and functional axis of the human body. It consists of 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae and is limited cranially by the skull and caudally by the sacrum.Vertebral Column: Anatomy. EnthesopathyEnthesopathyReactive Arthritis and dactylitisDactylitisAnkylosing Spondylitis are also seen. The diagnosis is clinical, and the condition should be suspected in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with psoriasisPsoriasisPsoriasis is a common T-cell-mediated inflammatory skin condition. The etiology is unknown, but is thought to be due to genetic inheritance and environmental triggers. There are 4 major subtypes, with the most common form being chronic plaque psoriasis. Psoriasis. Management includes DMARDsDMARDsDisease-modifying antirheumatic drugs are antiinflammatory medications used to manage rheumatoid arthritis. The medications slow, but do not cure, the progression of the disease. The medications are classified as either synthetic or biologic agents and each has unique mechanisms of action and side effects.Disease-Modifying Antirheumatic Drugs (DMARDs) and biologic agentsBiologic AgentsImmunosuppressants.
Ankylosing spondylitisAnkylosing spondylitisAnkylosing spondylitis (also known as Bechterew’s disease or Marie-Strümpell disease) is a seronegative spondyloarthropathy characterized by chronic and indolent inflammation of the axial skeleton. Severe disease can lead to fusion and rigidity of the spine. Ankylosing Spondylitis: a spondyloarthropathySpondyloarthropathyAnkylosing Spondylitis involving inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the axialAxialComputed Tomography (CT) skeleton, resulting in back painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, kyphosisKyphosisDeformities of the spine characterized by an exaggerated convexity of the vertebral column. The forward bending of the thoracic region usually is more than 40 degrees. This deformity sometimes is called round back or hunchback.Osteoporosis, and loss of lumbar lordosis. Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may also have peripheral joint involvement, anterior uveitisUveitisUveitis is the inflammation of the uvea, the pigmented middle layer of the eye, which comprises the iris, ciliary body, and choroid. The condition is categorized based on the site of disease; anterior uveitis is the most common. Diseases of the Uvea, aortic insufficiency, aortitisAortitisInflammation of the wall of the aorta.Ankylosing Spondylitis, cardiac conduction abnormalities, and cavitary lung lesions. Diagnosis is based on lumbosacral radiographic findings (sacroiliitisSacroiliitisInflammation of the sacroiliac joint. It is characterized by lower back pain, especially upon walking, fever, uveitis; psoriasis; and decreased range of motion. Many factors are associated with and cause sacroiliitis including infection; injury to spine, lower back, and pelvis; degenerative arthritis; and pregnancy.Ankylosing Spondylitis and “bamboo spineBamboo SpineAnkylosing Spondylitis”) and the presence of HLA-B27. Management includes NSAIDsNSAIDSPrimary vs Secondary Headaches, TNF inhibitorsTNF inhibitorsAnkylosing Spondylitis, or interleukin-17Interleukin-17A proinflammatory cytokine produced primarily by T-lymphocytes or their precursors. Several subtypes of interleukin-17 have been identified, each of which is a product of a unique gene.Interleukins antagonists.
Inflammatory bowel disease (IBD): includes Crohn’s disease and ulcerative colitisColitisInflammation of the colon section of the large intestine, usually with symptoms such as diarrhea (often with blood and mucus), abdominal pain, and fever.Pseudomembranous Colitis, and is characterized by chronic inflammationChronic InflammationInflammation of the GI tract due to a cell-mediated immune response to the GI mucosa. Symptoms include diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea, abdominal painAbdominal PainAcute Abdomen, and weight lossWeight lossDecrease in existing body weight.Bariatric Surgery. Extraintestinal manifestations can include a migratory peripheral arthritisPeripheral ArthritisReactive Arthritis of large joints. Inflammatory bowel disease is also associated with other disorders, such as ankylosing spondylitisAnkylosing spondylitisAnkylosing spondylitis (also known as Bechterew’s disease or Marie-Strümpell disease) is a seronegative spondyloarthropathy characterized by chronic and indolent inflammation of the axial skeleton. Severe disease can lead to fusion and rigidity of the spine. Ankylosing Spondylitis, sacroillitis, and uveitisUveitisUveitis is the inflammation of the uvea, the pigmented middle layer of the eye, which comprises the iris, ciliary body, and choroid. The condition is categorized based on the site of disease; anterior uveitis is the most common. Diseases of the Uvea. Diagnosis includes imaging, endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD), and biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma. Treatment involves steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors, aminosalicylates, immunomodulators, and biologic agentsBiologic AgentsImmunosuppressants
Billing and Coding
Diagnosis Codes:
This code is used to diagnose reactive arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis, an inflammatory arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis that develops in response to an infection elsewhere in the body, typically in the gastrointestinal or genitourinary tracts.
Coding System
Code
Description
ICD-10-CM
M02.3
Reiter’s disease
ICD-10-CM
M02.89
Other reactive arthropathies, multiple sites
Evaluation & Workup:
These codes are used to search for the preceding infection that triggered the arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis (e.g., chlamydiaChlamydiaChlamydiae are obligate intracellular gram-negative bacteria. They lack a peptidoglycan layer and are best visualized using Giemsa stain. The family of Chlamydiaceae comprises 3 pathogens that can infect humans: Chlamydia trachomatis, Chlamydia psittaci, and Chlamydia pneumoniae.Chlamydia testing) and to test for the HLA-B27 genetic marker, which is strongly associated with reactive arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis.
Coding System
Code
Description
CPT
87491
Infectious agent detection by nucleic acid (DNADNAA deoxyribonucleotide polymer that is the primary genetic material of all cells. Eukaryotic and prokaryotic organisms normally contain DNA in a double-stranded state, yet several important biological processes transiently involve single-stranded regions. DNA, which consists of a polysugar-phosphate backbone possessing projections of purines (adenine and guanine) and pyrimidines (thymine and cytosine), forms a double helix that is held together by hydrogen bonds between these purines and pyrimidines (adenine to thymine and guanine to cytosine).DNA Types and Structure or RNARNAA polynucleotide consisting essentially of chains with a repeating backbone of phosphate and ribose units to which nitrogenous bases are attached. RNA is unique among biological macromolecules in that it can encode genetic information, serve as an abundant structural component of cells, and also possesses catalytic activity.RNA Types and Structure); Chlamydia trachomatisChlamydia trachomatisType species of Chlamydia causing a variety of ocular and urogenital diseases.Chlamydia, amplified probeProbeA device placed on the patient’s body to visualize a targetUltrasound (Sonography) technique
CPT
86812
HLA typing; A, B, or C, single antigenAntigenSubstances that are recognized by the immune system and induce an immune reaction.Vaccination
Medications:
This code is for nonsteroidal anti-inflammatory drugs (NSAIDsNSAIDSPrimary vs Secondary Headaches) like naproxenNaproxenAn anti-inflammatory agent with analgesic and antipyretic properties. Both the acid and its sodium salt are used in the treatment of rheumatoid arthritis and other rheumatic or musculoskeletal disorders, dysmenorrhea, and acute gout.Nonsteroidal Antiinflammatory Drugs (NSAIDs), which are the first-line treatment to manage the joint painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of reactive arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis.
Coding System
Code
Description
RxNorm
7294
NaproxenNaproxenAn anti-inflammatory agent with analgesic and antipyretic properties. Both the acid and its sodium salt are used in the treatment of rheumatoid arthritis and other rheumatic or musculoskeletal disorders, dysmenorrhea, and acute gout.Nonsteroidal Antiinflammatory Drugs (NSAIDs) (ingredient)
Wendling, D., Prati, C., Chouk, M., Verhoeven, F. (2020). Reactive arthritis: treatment challenges and future perspectives. Current Rheumatology Reports, 22(7), 29. https://doi.org/10.1007/s11926-020-00904-9
Szamocki, S., Martyn-Hemphill, C., Green, J. S. A. (2016). Reactive arthritis: can’t see, can’t pee, can’t climb a tree…. Trends in Urology and Men’s Health, 7(1), 17–20. https://wchh.onlinelibrary.wiley.com/doi/10.1002/tre.501
Barber, C.E. (2013). Antibiotics for treatment of reactive arthritis: a systematic review and metaanalysis. Journal of Rheumatology, 40(6), 916–928. https://www.jrheum.org/content/40/6/916
Carlin, E. M., et al. (2014). 2014 European guideline on the management of sexually acquired reactive arthritis. International Journal of STD & AIDS, 25(13), 901–912. https://pubmed.ncbi.nlm.nih.gov/24974322/
Carlin, E., Marzo-Ortega, H., & Flew, S. (2021). British Association of Sexual Health and HIV national guideline on the management of sexually acquired reactive arthritis 2021. International journal of STD & AIDS, 32(11), 986–997. https://doi.org/10.1177/09564624211020266