Hypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5–5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake. If minor in severity, hypokalemia is usually asymptomatic. However, acute reductions in K+ level or severe hypokalemia can lead to cardiac arrhythmias, muscle weakness, rhabdomyolysis, paralysis, and respiratory failure. Diagnosis is by clinical history and lab testing. Management is guided by severity and includes treating urgent symptoms, replacing the K+ deficit, and treating the underlying cause.
PotassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia (K+) is the main intracellular cation in all cells and is distributed unevenly between the intracellular fluidIntracellular fluidThe fluid inside cells.Body Fluid Compartments (98%) and extracellular fluidExtracellular fluidThe fluid of the body that is outside of cells. It is the external environment for the cells.Body Fluid Compartments (2%). The large disparity is necessary for maintaining the resting membrane potentialResting membrane potentialMembrane Potential of cells.
The GI tract secretes 5%–10% of absorbed K+ daily.
KidneysKidneysThe kidneys are a pair of bean-shaped organs located retroperitoneally against the posterior wall of the abdomen on either side of the spine. As part of the urinary tract, the kidneys are responsible for blood filtration and excretion of water-soluble waste in the urine.Kidneys: Anatomy are responsible for 90%–95% of the overall K+ regulation and will severely limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation the excretion of K+ if intake is low.
Definition[10]
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia is defined as plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ concentration < 3.5 mEq/L.
Sites of action in the kidney[4,10,12]
Glomerulus: K+ is freely filtered.
Proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System: 65%–70% of filtered K+ is reabsorbed.
Thick ascending limbThick ascending limbRenal Sodium and Water Regulation of the loop of HenleLoop of HenleThe U-shaped portion of the renal tubule in the kidney medulla, consisting of a descending limb and an ascending limb. It is situated between the proximal kidney tubule and the distal kidney tubule.Tubular System: 10%–25% of filtered K+ is reabsorbed.
Principal cell (cortical collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma): K+ is secreted.
𝛼-intercalated cell (collecting ductCollecting ductStraight tubes commencing in the radiate part of the kidney cortex where they receive the curved ends of the distal convoluted tubules. In the medulla the collecting tubules of each pyramid converge to join a central tube (duct of bellini) which opens on the summit of the papilla.Renal Cell Carcinoma): K+ is reabsorbed.
The etiologies of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia can be grouped by 4 distinct mechanisms: poor dietary K+ intake, transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shift, GI losses, and renal losses.[1,2,4]
Poor dietary K+ intake:
Western diet: approximately 70–150 mmol K+/day
Uncommon cause outside of chronic malnutritionMalnutritionMalnutrition is a clinical state caused by an imbalance or deficiency of calories and/or micronutrients and macronutrients. The 2 main manifestations of acute severe malnutrition are marasmus (total caloric insufficiency) and kwashiorkor (protein malnutrition with characteristic edema).Malnutrition in children in resource-limited countries states (e.g., alcoholismAlcoholismA primary, chronic disease with genetic, psychosocial, and environmental factors influencing its development and manifestations. The disease is often progressive and fatal. It is characterized by impaired control over drinking, preoccupation with the drug alcohol, use of alcohol despite adverse consequences, and distortions in thinking, most notably denial. Each of these symptoms may be continuous or periodic.Wernicke Encephalopathy and Korsakoff Syndrome)
TranscellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shift:
Intracellular shifting of K+ results in hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
Factors increasing the intracellular shift:
InsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin
β2 adrenergic agonistsAdrenergic agonistsSympathomimetic drugs, also known as adrenergic agonists, mimic the action of the stimulators (î±, β, or dopamine receptors) of the sympathetic autonomic nervous system. Sympathomimetic drugs are classified based on the type of receptors the drugs act on (some agents act on several receptors but 1 is predominate).Sympathomimetic Drugs (e.g., albuterolAlbuterolA short-acting beta-2 adrenergic agonist that is primarily used as a bronchodilator agent to treat asthma.Sympathomimetic Drugs)
AlkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis: H+/K+ exchanger moves H+ out of the cell to help balance extracellular pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance in exchange for K+ moving into the cell to maintain electroneutrality.
GI losses: hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia develops due to downstream effects on the kidney:
Upper GI losses: HClHCLHairy cell leukemia (HCL) is a rare, chronic, B-cell leukemia characterized by the accumulation of small mature B lymphocytes that have “hair-like projections” visible on microscopy. The abnormal cells accumulate in the peripheral blood, bone marrow (causing fibrosis), and red pulp of the spleen, leading to cytopenias.Hairy Cell Leukemia is also in gastric fluid → metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis → contributes to hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia via transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifting:
VomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
LaxativeLaxativeAgents that produce a soft formed stool, and relax and loosen the bowels, typically used over a protracted period, to relieve constipation.Hypokalemia abuse
Villous adenomaVillous adenomaAn adenoma of the large intestine. It is usually a solitary, sessile, often large, tumor of colonic mucosa composed of mucinous epithelium covering delicate vascular projections. Hypersecretion and malignant changes occur frequently.Colorectal Cancer
Renal losses:
Metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis with high blood pressure:
↑ CortisolCortisolGlucocorticoids due to genetic conditions (congenital adrenal hyperplasiaHyperplasiaAn increase in the number of cells in a tissue or organ without tumor formation. It differs from hypertrophy, which is an increase in bulk without an increase in the number of cells.Cellular Adaptation, particularly 11β-hydroxylase deficiency11β-hydroxylase deficiencyCongenital Adrenal Hyperplasia and 17α-hydroxylase deficiency17α-hydroxylase deficiencyCongenital Adrenal Hyperplasia, which cause mineralocorticoid excessMineralocorticoid excessA hereditary disease characterized by childhood onset hypertension, hypokalemic alkalosis, and low renin and aldosterone secretion. It results from a defect in the activity of the 11-beta-hydroxysteroid dehydrogenase type 2 enzyme which results in inadequate conversion of cortisol to cortisone. The build up of unprocessed cortisol to levels that stimulate mineralocorticoid receptors creates the appearance of having excessive mineralocorticoids.Metabolic Alkalosis)
Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome
Metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis with low or normal blood pressure:
Loop and thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.HyponatremiadiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication: a significant cause of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia in outpatients and hospitalized patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship
Salt-wasting nephropathySalt-wasting nephropathyVolume Depletion and Dehydration (Bartter syndromeBartter syndromeBartter syndrome is a rare autosomal recessive disorder that affects the kidneys and presents either antenatally with severe or life-threatening manifestations or in childhood or adulthood with a milder course, depending on the genetic defect. Clinical disease results from defective renal reabsorption of sodium chloride in the thick ascending limb of the loop of Henle.Bartter Syndrome, Gitelman syndromeGitelman syndromeGitelman syndrome is a rare genetic autosomal recessive disorder that affects the sodium-chloride cotransporter in the distal convoluted tubule of the nephron and causes electrolyte abnormalities. The syndrome presents clinically with symptoms of hypokalemia and hypomagnesemia. Gitelman Syndrome)
Metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis:
Type 1Type 1Spinal Muscular Atrophy (distal) or type 2 (proximal) renal tubular acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis (RTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis)
Nonreabsorbable anionsAnionsNegatively charged atoms, radicals or groups of atoms which travel to the anode or positive pole during electrolysis.Electrolytes (e.g., 𝛽-hydroxybutyrate (diabetic ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis) or toluene sniffing (drug of abuse))
HypomagnesemiaHypomagnesemiaA nutritional condition produced by a deficiency of magnesium in the diet, characterized by anorexia, nausea, vomiting, lethargy, and weakness. Symptoms are paresthesias, muscle cramps, irritability, decreased attention span, and mental confusion, possibly requiring months to appear. Deficiency of body magnesium can exist even when serum values are normal. In addition, magnesium deficiency may be organ-selective, since certain tissues become deficient before others. Electrolytes:
Can directly cause hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
Can be due to diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea or diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication
Uncorrected hypomagnesemiaHypomagnesemiaA nutritional condition produced by a deficiency of magnesium in the diet, characterized by anorexia, nausea, vomiting, lethargy, and weakness. Symptoms are paresthesias, muscle cramps, irritability, decreased attention span, and mental confusion, possibly requiring months to appear. Deficiency of body magnesium can exist even when serum values are normal. In addition, magnesium deficiency may be organ-selective, since certain tissues become deficient before others. Electrolytes can make hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia correction due to any cause difficult.
Transcellular shift of K+:
Extracellular shift of K+:
1. Acidosis (increased H+) causes blockage of the Na+/H+ exchanger, which causes a decrease in intracellular Na+, in turn blocking Na+/K+ ATPase. On the other hand, acidosis activates the H+/K+ exchanger. Both cause an increase in extracellular K+.
2. Increased osmolarity in extracellular space (hyperglycemia, IV contrast, mannitol) shifts water outside the cell, decreasing K+ concentration. Increased gradient causes K+ diffusion outside.
Intracellular shift of K+:
1. Alkalosis (decreased H+) causes activation of the Na+/H+ exchanger, which causes an increase in intracellular Na+, in turn activating Na+/K+ ATPase. On the other hand, alkalosis blocks the H+/K+ exchanger. Both cause a decrease in extracellular K+.
2. Insulin and β2 adrenergic agonists activate Na+/K+ ATPase, lowering plasma K+ concentration.
Presentation of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia may include nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, constipationConstipationConstipation is common and may be due to a variety of causes. Constipation is generally defined as bowel movement frequency < 3 times per week. Patients who are constipated often strain to pass hard stools. The condition is classified as primary (also known as idiopathic or functional constipation) or secondary, and as acute or chronic. Constipation, skeletal muscle manifestations, and cardiac manifestations, which are potentially very serious. Symptoms are more likely to appear as the severity of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia increases, but patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may be asymptomatic even with relatively severe hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia.
Cardiac manifestations:[5,7,9]
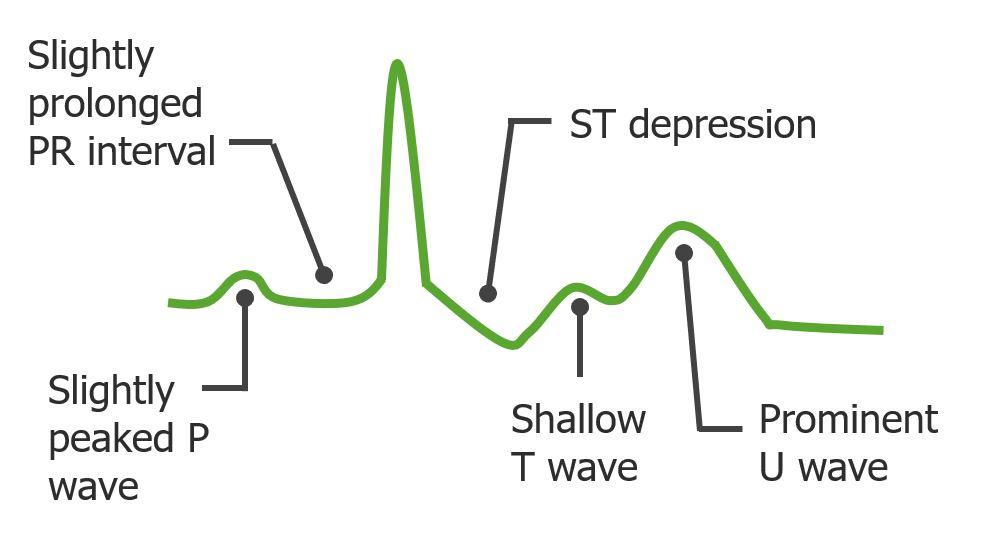
ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes:
PrematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis atrial/ventricular contractions
Atrioventricular blockAtrioventricular blockAtrioventricular (AV) block is a bradyarrhythmia caused by delay, or interruption, in the electrical conduction between the atria and the ventricles. Atrioventricular block occurs due to either anatomic or functional impairment, and is classified into 3 types. Atrioventricular block (AV block), sinus bradycardiaSinus bradycardiaBradyarrhythmias
Ventricular tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children and/or ventricular fibrillationVentricular fibrillationVentricular fibrillation (VF or V-fib) is a type of ventricular tachyarrhythmia (> 300/min) often preceded by ventricular tachycardia. In this arrhythmia, the ventricle beats rapidly and sporadically. The ventricular contraction is uncoordinated, leading to a decrease in cardiac output and immediate hemodynamic collapse. Ventricular Fibrillation (V-fib) if severe
Muscular symptoms:[5,10]
With mild-to-moderate hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia:
With severe hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia (< 2–2.5 mEq/L):
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may be asymptomatic even if severe hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia is present.
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis with an elevated serum CK level
IleusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction
Diagnostics and management may vary depending on practice location. The following information is based on US and UK guidelines and is geared toward the care of adult patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.
Diagnosis
General:[7,11]
Try to identify the cause of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia (e.g., GI losses, diuretic use).
If the etiology is clear from history, no further testing is needed.
However, ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) should be performed to assess for cardiac manifestations.
Blood tests:[3,7,10]
K+:
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia is defined as a serum K+ < 3.5 mEq/L.
Confirm with repeat measurement (particularly if level is surprisingly low).
Factors that can cause inaccurate results:
Very high WBC (e.g., leukemia) or recent IV insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin AND
Samples stored for long periods of time at room or high temperature
Mg2+ should always be checked to identify concomitant hypomagnesemiaHypomagnesemiaA nutritional condition produced by a deficiency of magnesium in the diet, characterized by anorexia, nausea, vomiting, lethargy, and weakness. Symptoms are paresthesias, muscle cramps, irritability, decreased attention span, and mental confusion, possibly requiring months to appear. Deficiency of body magnesium can exist even when serum values are normal. In addition, magnesium deficiency may be organ-selective, since certain tissues become deficient before others. Electrolytes.
Urine studies (performed if the etiology is unclear):[7,10,12]
Spot urine K+: frequently unreliable due to many possible confounding variablesConfounding variablesA confound is an additional variable other than the independent variable that has an effect on the dependent variable, causing an erroneous relationship to be inferred between them.Types of Biases:
> 15 mEq/L: renal loss
< 15 mEq/L: extrarenal loss (not always reliable, as diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia can result in secondary aldosteroneAldosteroneA hormone secreted by the adrenal cortex that regulates electrolyte and water balance by increasing the renal retention of sodium and the excretion of potassium.Hyperkalemia elevation → ↑ urinary K+)
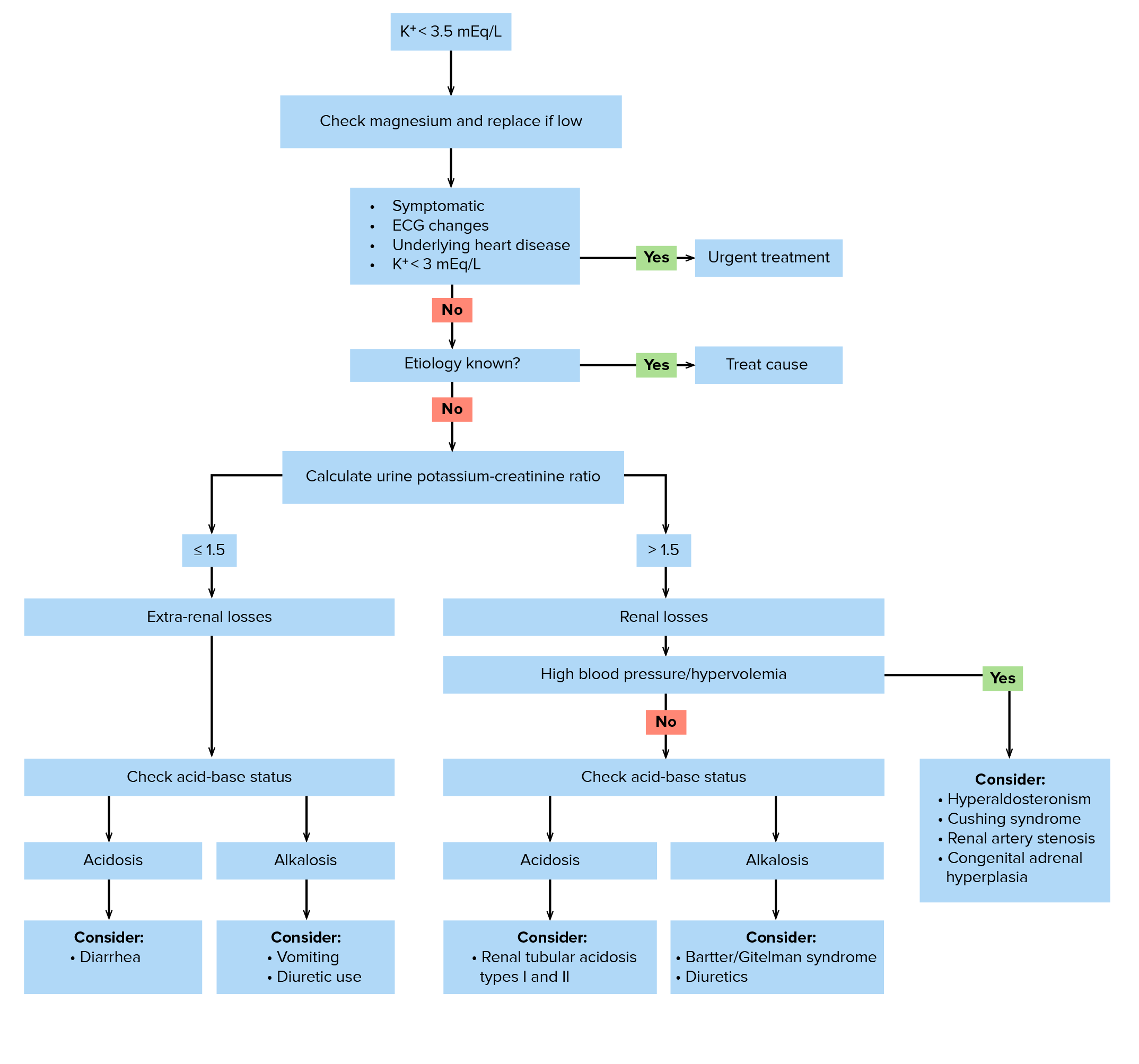
Urine potassium-creatinine ratio (more reliable than spot urine K+):
Adjusts for urine volume as creatinine is excreted at a near-constant rate
Correlates better with the 24-hour urine collection (impractical)
≤ 13 mEq/g creatinine (ratio ≤ 1.5) = extrarenal loss or transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shift:
If concurrent metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis → likely due to diarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea (including villous adenomaVillous adenomaAn adenoma of the large intestine. It is usually a solitary, sessile, often large, tumor of colonic mucosa composed of mucinous epithelium covering delicate vascular projections. Hypersecretion and malignant changes occur frequently.Colorectal Cancer or laxativeLaxativeAgents that produce a soft formed stool, and relax and loosen the bowels, typically used over a protracted period, to relieve constipation.Hypokalemia abuse)
If concurrent metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis→ likely due to vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia or diuretic use
> 13 mEq/g creatinine (ratio > 1.5) = renal loss:
If concurrent metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis → RTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis or nonreabsorbable anion (e.g., toluene inhalation)
If concurrent metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis, high blood pressure, and hypervolemiaHypervolemiaRenal Sodium and Water Regulation → may be due to mineralocorticoid excessMineralocorticoid excessA hereditary disease characterized by childhood onset hypertension, hypokalemic alkalosis, and low renin and aldosterone secretion. It results from a defect in the activity of the 11-beta-hydroxysteroid dehydrogenase type 2 enzyme which results in inadequate conversion of cortisol to cortisone. The build up of unprocessed cortisol to levels that stimulate mineralocorticoid receptors creates the appearance of having excessive mineralocorticoids.Metabolic Alkalosis, renal arteryRenal arteryA branch of the abdominal aorta which supplies the kidneys, adrenal glands and ureters.Glomerular FiltrationstenosisStenosisHypoplastic Left Heart Syndrome (HLHS), or Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome
Hypokalemia evaluation algorithm
Image by Lecturio.
Management
Treat urgent complications if present (seek help from an intensivist):[7–11]
Respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure
Brought on by skeletal and diaphragmatic muscle weakness
In rare severe cases, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may require noninvasive ventilationVentilationThe total volume of gas inspired or expired per unit of time, usually measured in liters per minute.Ventilation: Mechanics of Breathing.
Requires urgent correction of underlying hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
Arrhythmia: increased risk occurs with:
Increasing severity of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia (particularly < 2.5 mEq/L)
Concurrent hypomagnesemiaHypomagnesemiaA nutritional condition produced by a deficiency of magnesium in the diet, characterized by anorexia, nausea, vomiting, lethargy, and weakness. Symptoms are paresthesias, muscle cramps, irritability, decreased attention span, and mental confusion, possibly requiring months to appear. Deficiency of body magnesium can exist even when serum values are normal. In addition, magnesium deficiency may be organ-selective, since certain tissues become deficient before others. Electrolytes
Concurrent digoxinDigoxinA cardiotonic glycoside obtained mainly from digitalis lanata; it consists of three sugars and the aglycone digoxigenin. Digoxin has positive inotropic and negative chronotropic activity. It is used to control ventricular rate in atrial fibrillation and in the management of congestive heart failure with atrial fibrillation. Its use in congestive heart failure and sinus rhythm is less certain. The margin between toxic and therapeutic doses is small.Cardiac Glycosides or antiarrhythmic drug
Older age
Electrolyte replacement:[7,8,10,11]
Mild to moderately severe: oral KCl or potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia citrate
Serum K+ concentration declines by approximately 0.3 mEq/L for every 100 mEq reduction in total body K+ (e.g., a K+ drop from 3.8 to 2.9 mEq/L corresponds to a 300 mEq reduction in total bodyK+).
For low-normal levels → can increase dietary K+ intake
Otherwise, consider K+ supplementation:
Usual dose: 40–100 mEq in divided doses (usually 2–4 times per day) over 3–10 days
Reduce dose in renal insufficiency because there is a risk of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia.
For prophylaxisProphylaxisCephalosporins of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with ongoing losses, 20 mEq/day is sufficient.
Side effects include nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia; hence, complianceComplianceDistensibility measure of a chamber such as the lungs (lung compliance) or bladder. Compliance is expressed as a change in volume per unit change in pressure.Veins: Histology is often poor.
Severe (< 3 mEq/L, urgent symptoms, ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes, or if unable to take by mouth): IV K+
Standard concentration: 20–40 mEq/L in normal salineNormal salineA crystalloid solution that contains 9. 0g of sodium chloride per liter of water. It has a variety of uses, including: as a contact lens solution, in ophthalmic solutions and nasal lavage, in wound irrigation, and for fluid therapy.Intravenous Fluids
Maximal rate of infusion:
10 mEq/hr through peripheral IV
20 mEq/hr through a central line (typically used only in intensive care/emergency situations)
Continuous cardiac monitoring is indicated if the rate exceeds 10 mEq/hour
Fast rates of infusion can cause painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and irritation to the peripheral veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology (phlebitisPhlebitisInflammation of a vein, often a vein in the leg. Phlebitis associated with a blood clot is called (thrombophlebitis).Glycopeptides) → regularly check infusion site for rednessRednessInflammation and inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Note: KCl should not be mixed in 5% dextroseDextroseIntravenous Fluids in water (causes insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin release → transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shift of K+ leading to worsening hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia).
Replace magnesiumMagnesiumA metallic element that has the atomic symbol mg, atomic number 12, and atomic weight 24. 31. It is important for the activity of many enzymes, especially those involved in oxidative phosphorylation.Electrolytes if low → concurrent hypomagnesemiaHypomagnesemiaA nutritional condition produced by a deficiency of magnesium in the diet, characterized by anorexia, nausea, vomiting, lethargy, and weakness. Symptoms are paresthesias, muscle cramps, irritability, decreased attention span, and mental confusion, possibly requiring months to appear. Deficiency of body magnesium can exist even when serum values are normal. In addition, magnesium deficiency may be organ-selective, since certain tissues become deficient before others. Electrolytes can:
Exacerbate rhythm disturbances
Impede adequate K+ replacement
Monitoring[7,9,11]
Important at all levels of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia:
Cardiac monitoring:
Serial ECGs and/or continuous cardiac monitoring (i.e., telemetryTelemetryTransmission of the readings of instruments to a remote location by means of wires, radio waves, or other means.Crush Syndrome)
Some patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship will not have signs of arrhythmia or ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) changes even with severe hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia.
Lab monitoring:
Repeat serum K+ frequently based on the severity of hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia and the clinical situation.
GlucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance monitoring for hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia
Treat the underlying disease (potassium-sparing diuretic may be required):[7,10,11]
Bartter syndromeBartter syndromeBartter syndrome is a rare autosomal recessive disorder that affects the kidneys and presents either antenatally with severe or life-threatening manifestations or in childhood or adulthood with a milder course, depending on the genetic defect. Clinical disease results from defective renal reabsorption of sodium chloride in the thick ascending limb of the loop of Henle.Bartter Syndrome or Gitelman syndromeGitelman syndromeGitelman syndrome is a rare genetic autosomal recessive disorder that affects the sodium-chloride cotransporter in the distal convoluted tubule of the nephron and causes electrolyte abnormalities. The syndrome presents clinically with symptoms of hypokalemia and hypomagnesemia. Gitelman Syndrome: amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome
Primary aldosteronism: spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics
RhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis:potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia may be normal or high on presentation due to the release of intracellular K+ as muscle cells die. Because many causes of rhabdomyolysisRhabdomyolysisRhabdomyolysis is characterized by muscle necrosis and the release of toxic intracellular contents, especially myoglobin, into the circulation.Rhabdomyolysis exist other than hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia and the risk of hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia with overaggressive K+ replacement is significant, only replace K+ if and when plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products levels are low. Diagnosis is made by history and CK levels, and management of the underlying cause is needed.
Diabetic ketoacidosisKetoacidosisA life-threatening complication of diabetes mellitus, primarily of type 1 diabetes mellitus with severe insulin deficiency and extreme hyperglycemia. It is characterized by ketosis; dehydration; and depressed consciousness leading to coma.Metabolic Acidosis (DKADKADiabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are serious, acute complications of diabetes mellitus. Diabetic ketoacidosis is characterized by hyperglycemia and ketoacidosis due to an absolute insulin deficiency. Hyperglycemic Crises): presents with K+ deficit of the total body (urinary losses from osmotic diuresisOsmotic diuresisVolume Depletion and Dehydration/polyuriaPolyuriaUrination of a large volume of urine with an increase in urinary frequency, commonly seen in diabetes.Renal Potassium Regulation); however, plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ is normal or high due to severe transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifting from insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin deficiency. Diagnosis is made by history and lab testing, which include glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance and serum ketonesKetonesOrganic compounds containing a carbonyl group =C=O bonded to two hydrocarbon groups.Basics of Carbohydrates. Treatment includes starting an insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin drip and replacing K+ once the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products level falls to 4.5 mEq/L since the intracellular shift will cause hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia.
Hypokalemic periodic paralysisHypokalemic Periodic ParalysisAn autosomal dominant familial disorder characterized by recurrent episodes of skeletal muscle weakness associated with falls in serum potassium levels. The condition usually presents in the first or second decade of life with attacks of trunk and leg paresis during sleep or shortly after awakening. Symptoms may persist for hours to days and generally are precipitated by exercise or a meal high in carbohydrates.Ion Channel Myopathy: characterized by acute attacks of muscle weakness and/or paralysis precipitated by rest after exercise, stress, and/or a high-carbohydrate meal. Hypokalemic periodic paralysisHypokalemic Periodic ParalysisAn autosomal dominant familial disorder characterized by recurrent episodes of skeletal muscle weakness associated with falls in serum potassium levels. The condition usually presents in the first or second decade of life with attacks of trunk and leg paresis during sleep or shortly after awakening. Symptoms may persist for hours to days and generally are precipitated by exercise or a meal high in carbohydrates.Ion Channel Myopathy can be genetic or acquired (associated with hyperthyroidismHyperthyroidismHypersecretion of thyroid hormones from the thyroid gland. Elevated levels of thyroid hormones increase basal metabolic rate.Thyrotoxicosis and Hyperthyroidism/thyrotoxicosisThyrotoxicosisA hypermetabolic syndrome caused by excess thyroid hormones which may come from endogenous or exogenous sources. The endogenous source of hormone may be thyroid hyperplasia; thyroid neoplasms; or hormone-producing extrathyroidal tissue. Thyrotoxicosis is characterized by nervousness; tachycardia; fatigue; weight loss; heat intolerance; and excessive sweating.Thyrotoxicosis and Hyperthyroidism). Hypokalemic periodic paralysisHypokalemic Periodic ParalysisAn autosomal dominant familial disorder characterized by recurrent episodes of skeletal muscle weakness associated with falls in serum potassium levels. The condition usually presents in the first or second decade of life with attacks of trunk and leg paresis during sleep or shortly after awakening. Symptoms may persist for hours to days and generally are precipitated by exercise or a meal high in carbohydrates.Ion Channel Myopathy is the prototypical disease due to severe transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifting of K+. The presentation includes a plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products K+ decrease to 1.5–2.5 mEq/L. Supplemental K+ should only be replaced if symptomatic and done cautiously given the risk for rebound hyperkalemiaHyperkalemiaHyperkalemia is defined as a serum potassium (K+) concentration >5.2 mEq/L. Homeostatic mechanisms maintain the serum K+ concentration between 3.5 and 5.2 mEq/L, despite marked variation in dietary intake. Hyperkalemia can be due to a variety of causes, which include transcellular shifts, tissue breakdown, inadequate renal excretion, and drugs. Hyperkalemia once the transcellularTranscellularThe movement of one cell into, through, and out of another cell.Tubular System shifting is corrected.
Chronic hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia: can have long-term adverse effects, including worsening hypertensionHypertensionHypertension, or high blood pressure, is a common disease that manifests as elevated systemic arterial pressures. Hypertension is most often asymptomatic and is found incidentally as part of a routine physical examination or during triage for an unrelated medical encounter. Hypertension, chronic kidney diseaseChronic Kidney DiseaseChronic kidney disease (CKD) is kidney impairment that lasts for ≥ 3 months, implying that it is irreversible. Hypertension and diabetes are the most common causes; however, there are a multitude of other etiologies. In the early to moderate stages, CKD is usually asymptomatic and is primarily diagnosed by laboratory abnormalities.Chronic Kidney Disease, and polyuriaPolyuriaUrination of a large volume of urine with an increase in urinary frequency, commonly seen in diabetes.Renal Potassium Regulation. Chronic hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia may increase the risk of developing diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus in conjunction with thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.HyponatremiadiureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication.
False-positive hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia: a common occurrence in hospital settings, usually caused by blood drawn from an IV nearby a hypotonicHypotonicSolutions that have a lesser osmotic pressure than a reference solution such as blood, plasma, or interstitial fluid.Renal Sodium and Water Regulation fluid infusion. Cells in the blood can also have significant uptake of K+ if the blood sample is left in warm temperatures for a prolonged period of time, or if the WBC is very high (e.g., > 100,000/mL in leukemia).
Salt-wasting nephropathies:Bartter syndromeBartter syndromeBartter syndrome is a rare autosomal recessive disorder that affects the kidneys and presents either antenatally with severe or life-threatening manifestations or in childhood or adulthood with a milder course, depending on the genetic defect. Clinical disease results from defective renal reabsorption of sodium chloride in the thick ascending limb of the loop of Henle.Bartter Syndrome and Gitelman syndromeGitelman syndromeGitelman syndrome is a rare genetic autosomal recessive disorder that affects the sodium-chloride cotransporter in the distal convoluted tubule of the nephron and causes electrolyte abnormalities. The syndrome presents clinically with symptoms of hypokalemia and hypomagnesemia. Gitelman Syndrome with a clinical presentation of metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis, low or normal blood pressure, and hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia from renal losses. Both are rare, autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance syndromes; however, the mechanism of Bartter syndromeBartter syndromeBartter syndrome is a rare autosomal recessive disorder that affects the kidneys and presents either antenatally with severe or life-threatening manifestations or in childhood or adulthood with a milder course, depending on the genetic defect. Clinical disease results from defective renal reabsorption of sodium chloride in the thick ascending limb of the loop of Henle.Bartter Syndrome resembles a loop diuretic and the mechanism of Gitelman syndromeGitelman syndromeGitelman syndrome is a rare genetic autosomal recessive disorder that affects the sodium-chloride cotransporter in the distal convoluted tubule of the nephron and causes electrolyte abnormalities. The syndrome presents clinically with symptoms of hypokalemia and hypomagnesemia. Gitelman Syndrome resembles a thiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.Hyponatremia diuretic. Treatment includes a potassium-sparing diuretic (spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics or amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome) and NSAIDsNSAIDSPrimary vs Secondary Headaches.
Liddle syndromeLiddle syndromeLiddle syndrome, a type of pseudohyperaldosteronism, is a rare cause of secondary hypertension. Liddle syndrome results from autosomal dominant gain-of-function mutations in the genes that encode the epithelial sodium channel (ENaC) subunits, also known as the “collecting tubule sodium channel” or “amiloride-sensitive sodium channel.” The activity of ENAC is increased, leading to sodium and water retention. Liddle Syndrome: a rare, autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance disease presenting clinically with metabolic alkalosisAlkalosisA pathological condition that removes acid or adds base to the body fluids.Respiratory Alkalosis, high blood pressure, and hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia from renal losses. Treatment includes a potassium-sparing diuretic (amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome or triamtereneTriamtereneA pteridinetriamine compound that inhibits sodium reabsorption through sodium channels in renal epithelial cells.Potassium-sparing Diuretics).
Type 1Type 1Spinal Muscular AtrophyRTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis (also known as distalRTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis): the condition results in systemic metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis due to impaired distal acidification in the kidney. Distal RTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis can be genetic or acquired (due to drugs or autoimmune disease). Diagnosis is made on history and lab testing. Treatment is oral bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes, usually in the form of sodiumSodiumA member of the alkali group of metals. It has the atomic symbol na, atomic number 11, and atomic weight 23.HyponatremiabicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes or potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia citrate.
Type 2 RTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis (also known as proximalRTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis): the condition results in systemic metabolic acidosisAcidosisA pathologic condition of acid accumulation or depletion of base in the body. The two main types are respiratory acidosis and metabolic acidosis, due to metabolic acid build up.Respiratory Acidosis due to impaired reabsorption of filtered bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes in the proximal tubuleProximal tubuleThe renal tubule portion that extends from the bowman capsule in the kidney cortex into the kidney medulla. The proximal tubule consists of a convoluted proximal segment in the cortex, and a distal straight segment descending into the medulla where it forms the u-shaped loop of henle.Tubular System. Proximal RTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis can be genetic or acquired (i.e., due to drugs or multiple myeloma). Diagnosis is made on history and lab testing. Treatment is more complicated than type 1Type 1Spinal Muscular AtrophyRTARTARenal tubular acidosis (RTA) is an imbalance in physiologic pH caused by the kidney’s inability to acidify urine to maintain blood pH at physiologic levels. Renal tubular acidosis exist in multiple types, including distal RTA (type 1), proximal RTA (type 2), and hyperkalemic RTA (type 4). Renal Tubular Acidosis and involves a combination of oral bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes, oral K+ supplementation, hydrochlorothiazideHydrochlorothiazideA thiazide diuretic often considered the prototypical member of this class. It reduces the reabsorption of electrolytes from the renal tubules. This results in increased excretion of water and electrolytes, including sodium, potassium, chloride, and magnesium. It is used in the treatment of several disorders including edema, hypertension, diabetes insipidus, and hypoparathyroidism.Thiazide Diuretics, and a potassium-sparing diuretic (amilorideAmilorideA pyrazine compound inhibiting sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Amiloride is used in conjunction with diuretics to spare potassium loss.Liddle Syndrome or spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics).
Nonreabsorbable anions: anions (e.g., 𝛽-hydroxybutyrate, hippurate) associated with metabolic acidosis cause hypokalemia from increased renal excretion of K+. Ketoacidosis can result from uncontrolled diabetes, starvation, or alcoholism and is associated with high 𝛽-hydroxybutyrate levels. Hippurate is a metabolite of toluene, which is found in paint thinner, and inhaled as a drug of abuse (“huffing”).
Billing and Coding
Diagnosis Codes:
This code is used to formally document hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia, a condition characterized by a lower-than-normal level of potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia in the bloodstream.
Coding System
Code
Description
ICD-10-CM
E87.6
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia
SNOMED CT
4669009
HypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia (disorder)
Evaluation & Workup:
These codes are used to order a metabolic panel to confirm the low potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia level and assess other electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes and kidney function, as well as an ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) to check for characteristic changes caused by hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia.
ElectrocardiogramElectrocardiogramAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG), routine ECGECGAn electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart plotted against time. Adhesive electrodes are affixed to the skin surface allowing measurement of cardiac impulses from many angles. The ECG provides 3-dimensional information about the conduction system of the heart, the myocardium, and other cardiac structures. Electrocardiogram (ECG) with at least 12 leads; with interpretation and report
Medications:
These codes are for medications used to treat hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia. Potassium chloridePotassium chlorideA white crystal or crystalline powder used in buffers; fertilizers; and explosives. It can be used to replenish electrolytes and restore water-electrolyte balance in treating hypokalemia.Esophagitis is used for direct replacement, while spironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics, a potassium-sparing diuretic, may be used if the potassiumPotassiumAn element in the alkali group of metals with an atomic symbol k, atomic number 19, and atomic weight 39. 10. It is the chief cation in the intracellular fluid of muscle and other cells. Potassium ion is a strong electrolyte that plays a significant role in the regulation of fluid volume and maintenance of the water-electrolyte balance.Hyperkalemia loss is medication-induced.
Coding System
Code
Description
RxNorm
8593
Potassium ChloridePotassium chlorideA white crystal or crystalline powder used in buffers; fertilizers; and explosives. It can be used to replenish electrolytes and restore water-electrolyte balance in treating hypokalemia.Esophagitis (ingredient)
RxNorm
9997
SpironolactoneSpironolactoneA potassium sparing diuretic that acts by antagonism of aldosterone in the distal renal tubules. It is used mainly in the treatment of refractory edema in patients with congestive heart failure, nephrotic syndrome, or hepatic cirrhosis. Its effects on the endocrine system are utilized in the treatments of hirsutism and acne but they can lead to adverse effects.Potassium-sparing Diuretics (ingredient)
ATC
A12BA01
Potassium chloridePotassium chlorideA white crystal or crystalline powder used in buffers; fertilizers; and explosives. It can be used to replenish electrolytes and restore water-electrolyte balance in treating hypokalemia.Esophagitis
Complications:
These codes document the most serious complications of severe hypokalemiaHypokalemiaHypokalemia is defined as plasma potassium (K+) concentration < 3.5 mEq/L. Homeostatic mechanisms maintain plasma concentration between 3.5-5.2 mEq/L despite marked variation in dietary intake. Hypokalemia can be due to renal losses, GI losses, transcellular shifts, or poor dietary intake.Hypokalemia, including potentially life-threatening cardiac arrhythmias and significant muscle weakness.
Liamis, G., Liberopoulos, E., Barkas, F., & Elisaf, M. (2013). Spurious electrolyte disorders: A diagnostic challenge for clinicians. American Journal of Nephrology. 38(1), 50–57. https://doi.org/10.1159/000351804