Gastrointestinal bleeding indicates underlying pathology in either the upper or lower gastrointestinal (GI) tract. Hematemesis (vomiting red blood or “coffee-ground” material) and melena (black, tarry stool) usually indicate upper GI bleeding proximal to the suspensory ligament of the duodenum, also called the ligament of Treitz. Peptic ulcer disease (PUD) is the most common cause of upper GI bleeding. Hematochezia (red blood in the stool) is most often associated with lower GI bleeding (although it infrequently occurs with massive upper GI bleeding that is typically associated with hypotension). Lower GI bleeding can be from diverticular disease, angiodysplasia, polyps or tumors, inflammatory bowel disease, or internal hemorrhoids. Diagnosis is made by clinical history and physical exam, followed by upper and/or lower GI endoscopy. The source of the bleeding can usually be identified and treated with endoscopy.
Upper gastrointestinal bleedingGastrointestinal bleedingGastrointestinal bleeding (GIB) is a symptom of multiple diseases within the gastrointestinal (GI) tract. Gastrointestinal bleeding is designated as upper or lower based on the etiology’s location to the ligament of Treitz. Depending on the location of the bleeding, the patient may present with hematemesis (vomiting blood), melena (black, tarry stool), or hematochezia (fresh blood in stools). Gastrointestinal Bleeding (UGIB):[2,16]
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: about 65 per 100,000 adults per year
Twice as common in men
Increased risk with age (> 60 years)
Lower gastrointestinal bleedingGastrointestinal bleedingGastrointestinal bleeding (GIB) is a symptom of multiple diseases within the gastrointestinal (GI) tract. Gastrointestinal bleeding is designated as upper or lower based on the etiology’s location to the ligament of Treitz. Depending on the location of the bleeding, the patient may present with hematemesis (vomiting blood), melena (black, tarry stool), or hematochezia (fresh blood in stools). Gastrointestinal Bleeding (LGIB):[8]
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: estimated at 33‒87 per 100,000 adults
Increased risk with age (200-fold increase in the 3rd–9th decades)
Somewhat more common in men
Risk factors:
UGIB:
Helicobacter pyloriHelicobacter pyloriA spiral bacterium active as a human gastric pathogen. It is a gram-negative, urease-positive, curved or slightly spiral organism initially isolated in 1982 from patients with lesions of gastritis or peptic ulcers in Western Australia. Helicobacter pylori was originally classified in the genus campylobacter, but RNA sequencing, cellular fatty acid profiles, growth patterns, and other taxonomic characteristics indicate that the micro-organism should be included in the genus Helicobacter. It has been officially transferred to Helicobacter gen.Helicobacter infection
CirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis
LGIB: vascular disease
Both UGIB and LGIB:
NSAIDNSAIDNonsteroidal antiinflammatory drugs (NSAIDs) are a class of medications consisting of aspirin, reversible NSAIDs, and selective NSAIDs. NSAIDs are used as antiplatelet, analgesic, antipyretic, and antiinflammatory agents. Nonsteroidal Antiinflammatory Drugs (NSAIDs) use
Alcohol use
SmokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Most common causes: gastric and duodenal ulcers (PUDPUDPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease)
EsophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
Esophageal varices
EsophagitisEsophagitisEsophagitis is the inflammation or irritation of the esophagus. The major types of esophagitis are medication-induced, infectious, eosinophilic, corrosive, and acid reflux. Patients typically present with odynophagia, dysphagia, and retrosternal chest pain. Esophagitis: infection or inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation in the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy
Esophageal cancerEsophageal cancerEsophageal cancer is 1 of the most common causes of cancer-related deaths worldwide. Nearly all esophageal cancers are either adenocarcinoma (commonly affecting the distal esophagus) or squamous cell carcinoma (affecting the proximal two-thirds of the esophagus). Esophageal Cancer
Mallory-Weiss tearMallory-Weiss TearMallory-Weiss syndrome (MWS) is defined by the presence of longitudinal mucosal lacerations in the distal esophagus and proximal stomach, which are usually associated with any action that provokes a sudden rise in intraluminal esophageal pressure, such as forceful or recurrent retching, vomiting, coughing, or straining. Mallory-Weiss Syndrome (Mallory-Weiss Tear): a tear in the esophageal lining due to forceful vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
StomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy
Gastric ulcerGastric ulcerUlceration of the gastric mucosa due to contact with gastric juice. It is often associated with Helicobacter pylori infection or consumption of nonsteroidal anti-inflammatory drugs (NSAIDS).Peptic Ulcer Disease
Erosive gastritisGastritisGastritis refers to inflammation of the gastric mucosa. Gastritis may occur suddenly (acute gastritis) or slowly over time (chronic gastritis). Gastritis may be asymptomatic or with symptoms, including burning abdominal pain (which either worsens or improves with eating), dyspepsia, nausea, and vomiting. Gastritis
Gastric cancerGastric cancerGastric cancer is the 3rd-most common cause of cancer-related deaths worldwide. The majority of cases are from adenocarcinoma. The modifiable risk factors include Helicobacter pylori infection, smoking, and nitrate-rich diets. Gastric Cancer
Gastric antral vascular ectasiaGastric Antral Vascular EctasiaA distinct vascular lesion in the pyloric antrum that is characterized by tortuous dilated blood vessels (ectasia) radiating outward from the pylorus. The vessel pattern resembles the stripes on the surface of a watermelon. This lesion causes both acute and chronic gastrointestinal hemorrhage.Gastrointestinal Bleeding (GAVE): dilated small blood vessels in the pyloric antrum (uncommon)
Dieulafoy lesionDieulafoy lesionVascular malformation in the stomach (submucosa) that ulcerates and causes massive bleedingPeptic Ulcer Disease: a large, tortuous vessel that can erode and bleed
AngiodysplasiaAngiodysplasiaAcquired degenerative dilation or expansion (ectasia) of normal blood vessels, often associated with aging. They are isolated, tortuous, thin-walled vessels and sources of bleeding. They occur most often in mucosal capillaries of the gastrointestinal tract leading to gastrointestinal hemorrhage and anemia.Gastrointestinal Bleeding: an abnormal collection of blood vessels
DuodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy
AngiodysplasiaAngiodysplasiaAcquired degenerative dilation or expansion (ectasia) of normal blood vessels, often associated with aging. They are isolated, tortuous, thin-walled vessels and sources of bleeding. They occur most often in mucosal capillaries of the gastrointestinal tract leading to gastrointestinal hemorrhage and anemia.Gastrointestinal Bleeding
Cancer
Aortoenteric fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula (rare)
The source of bleeding is not identified in up to 10%‒15% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship.[16]
Diverticular diseaseDiverticular diseaseDiverticula are protrusions of the bowel wall occurring most commonly in the colon. The condition of having diverticula (called diverticulosis) is mostly asymptomatic. These diverticula can become symptomatic, however, when associated with diseases. Diverticulitis is the inflammation of diverticula, often presenting with lower abdominal pain and changes in bowel habits.Diverticular Disease
DiverticulosisDiverticulosisA pathological condition characterized by the presence of a number of colonic diverticula in the colon. Its pathogenesis is multifactorial, including colon aging, motor dysfunction, increases in intraluminal pressure, and lack of dietary fibers.Diverticular Disease: sac-like protrusion of the colonic wall (common)
DiverticulitisDiverticulitisInflammation of a diverticulum or diverticula.Diverticular Disease: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation/infection of diverticula (less commonly associated with GI bleed)
Meckel diverticulumDiverticulumA pouch or sac opening from the colon.Diverticular Disease: congenital outpouching in the ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy
Vascular disease
AngiodysplasiaAngiodysplasiaAcquired degenerative dilation or expansion (ectasia) of normal blood vessels, often associated with aging. They are isolated, tortuous, thin-walled vessels and sources of bleeding. They occur most often in mucosal capillaries of the gastrointestinal tract leading to gastrointestinal hemorrhage and anemia.Gastrointestinal Bleeding
IschemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage (e.g., mesenteric ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage, ischemic colitisIschemic colitisInflammation of the colon due to colonic ischemia resulting from alterations in systemic circulation or local vasculature.Large Bowel Obstruction)
Internal hemorrhoidsHemorrhoidsHemorrhoids are normal vascular cushions in the anal canal composed of dilated vascular tissue, smooth muscle, and connective tissue. They do not cause issues unless they are enlarged, inflamed, thrombosed, or prolapsed. Patients often present with rectal bleeding of bright red blood, or they may have pain, perianal pruritus, or a palpable mass. Hemorrhoids: venous structures of the anorectum that engorge, prolapse, and bleed
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy polyp
Colorectal cancerColorectal cancerColorectal cancer (CRC) is the 2nd leading cause of cancer-related deaths in the United States. Colorectal cancer is a heterogeneous disease that arises from genetic and epigenetic abnormalities, with influence from environmental factors. Colorectal Cancer
Inflammatory disease
Infectious colitisColitisInflammation of the colon section of the large intestine, usually with symptoms such as diarrhea (often with blood and mucus), abdominal pain, and fever.Pseudomembranous Colitis
Inflammatory bowel disease: ulcerative colitisColitisInflammation of the colon section of the large intestine, usually with symptoms such as diarrhea (often with blood and mucus), abdominal pain, and fever.Pseudomembranous Colitis and Crohn disease
IatrogenicIatrogenicAny adverse condition in a patient occurring as the result of treatment by a physician, surgeon, or other health professional, especially infections acquired by a patient during the course of treatment.Anterior Cord Syndrome
After biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma or polypectomy
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).OsteosarcomacolitisColitisInflammation of the colon section of the large intestine, usually with symptoms such as diarrhea (often with blood and mucus), abdominal pain, and fever.Pseudomembranous Colitis: radiation-induced inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation in the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
Aortoenteric fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula (rare, but serious)
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with occult bleeding may be asymptomatic.
Symptoms of anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types:
FatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia, weakness
DyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea
SyncopeSyncopeSyncope is a short-term loss of consciousness and loss of postural stability followed by spontaneous return of consciousness to the previous neurologic baseline without the need for resuscitation. The condition is caused by transient interruption of cerebral blood flow that may be benign or related to a underlying life-threatening condition. Syncope
Abdominal painAbdominal PainAcute Abdomen or heartburnHeartburnSubsternal pain or burning sensation, usually associated with regurgitation of gastric juice into the esophagus.Gastroesophageal Reflux Disease (GERD) → ulcers, gastritisGastritisGastritis refers to inflammation of the gastric mucosa. Gastritis may occur suddenly (acute gastritis) or slowly over time (chronic gastritis). Gastritis may be asymptomatic or with symptoms, including burning abdominal pain (which either worsens or improves with eating), dyspepsia, nausea, and vomiting. Gastritis, ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage
UGIB:
Coffee-ground emesis
HematemesisHematemesisVomiting of blood that is either fresh bright red, or older ‘coffee-ground’ in character. It generally indicates bleeding of the upper gastrointestinal tract.Mallory-Weiss Syndrome (Mallory-Weiss Tear)
Rarely, may be due to bleeding from the cecumCecumThe blind sac or outpouching area of the large intestine that is below the entrance of the small intestine. It has a worm-like extension, the vermiform appendix.Colon, Cecum, and Appendix: Anatomy or right colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy[3]
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with mild or occult bleeding may not have significant findings.
Evidence of hemodynamic instability:
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension
Orthostatic hypotensionOrthostatic hypotensionA significant drop in blood pressure after assuming a standing position. Orthostatic hypotension is a finding, and defined as a 20-mm hg decrease in systolic pressure or a 10-mm hg decrease in diastolic pressure 3 minutes after the person has risen from supine to standing. Symptoms generally include dizziness, blurred vision, and syncope.Hypotension: seen with acute blood loss of ≥ 2 units
Pale skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions color and conjunctivaConjunctivaThe mucous membrane that covers the posterior surface of the eyelids and the anterior pericorneal surface of the eyeball.Eye: Anatomy
Some may have abdominal tenderness (e.g., ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage).
Rectal exam:
Black or bloody stools
Normal, brown stool may be seen with occult bleeding
HemorrhoidsHemorrhoidsHemorrhoids are normal vascular cushions in the anal canal composed of dilated vascular tissue, smooth muscle, and connective tissue. They do not cause issues unless they are enlarged, inflamed, thrombosed, or prolapsed. Patients often present with rectal bleeding of bright red blood, or they may have pain, perianal pruritus, or a palpable mass. Hemorrhoids
Rectal massMassThree-dimensional lesion that occupies a space within the breastImaging of the Breast
Evaluate for signs of chronic liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease:
SplenomegalySplenomegalySplenomegaly is pathologic enlargement of the spleen that is attributable to numerous causes, including infections, hemoglobinopathies, infiltrative processes, and outflow obstruction of the portal vein. Splenomegaly
Abdominal distension and ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites
The approach to evaluating patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with GI bleeding depends on its severity and whether the patient is able to undergo endoscopic evaluation. Diagnosis and management are often approached concurrently.
May show mild or severe anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types from blood loss
Hemoglobin may initially be normal with acute bleeding.
Potential thrombocytopeniaThrombocytopeniaThrombocytopenia occurs when the platelet count is < 150,000 per microliter. The normal range for platelets is usually 150,000-450,000/µL of whole blood. Thrombocytopenia can be a result of decreased production, increased destruction, or splenic sequestration of platelets. Patients are often asymptomatic until platelet counts are < 50,000/µL. Thrombocytopenia may be seen in cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis.
Blood type and crossmatch (for a potential blood transfusion)
Fecal occult blood testing (FOBT):
Helps determine if black or red stool is due to bleeding (as opposed to other causes)
Black stools may be due to ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements supplements or bismuth.
Red stools may be due to food.
Negative FOBT supports other diagnoses.
Coagulation factorsCoagulation factorsEndogenous substances, usually proteins, that are involved in the blood coagulation process.Hemostasis: to check for coagulopathy; may need reversal
Liver function testsLiver function testsLiver function tests, also known as hepatic function panels, are one of the most commonly performed screening blood tests. Such tests are also used to detect, evaluate, and monitor acute and chronic liver diseases.Liver Function Tests: to check for underlying liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease
Basic metabolic panelBasic Metabolic PanelPrimary vs Secondary Headaches: ↑ blood ureaUreaA compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids.Urea CyclenitrogenNitrogenAn element with the atomic symbol n, atomic number 7, and atomic weight [14. 00643; 14. 00728]. Nitrogen exists as a diatomic gas and makes up about 78% of the earth’s atmosphere by volume. It is a constituent of proteins and nucleic acids and found in all living cells.Urea Cycle (BUN) may signal upper GIB
IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements, ferritinFerritinIron-containing proteins that are widely distributed in animals, plants, and microorganisms. Their major function is to store iron in a nontoxic bioavailable form. Each ferritin molecule consists of ferric iron in a hollow protein shell (apoferritins) made of 24 subunits of various sequences depending on the species and tissue types.Hereditary Hemochromatosis, total ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements binding capacity (TIBC): to evaluate for chronic ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements deficiency
Imaging[3,8,10]
Computed tomography with angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery (CTACTAA non-invasive method that uses a ct scanner for capturing images of blood vessels and tissues. A contrast material is injected, which helps produce detailed images that aid in diagnosing vascular diseases.Pulmonary Function Tests):
Bleeding must be at least 0.3–0.5 mL/min for detection
Uses IV contrast to localize the site of bleeding
Typically ordered in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with hemodynamic instability who are unable to undergo endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)[8,10]
Radionuclide imaging:
Bleeding must be at least 0.1–0.5 mL/min for detection.
Most sensitive radiographic test
Uses an injected radioisotope to identify sites of extravasation.
Procedures and interventions[3-8,10,20]
EndoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD):
Esophagoduodenoscopy (EGD):
Method of choice in UGIB
Visualize the site of hemorrhage within the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy, stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy, or duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy
Visualize the site of hemorrhage within the large intestineLarge intestineThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy and terminal ileumIleumThe distal and narrowest portion of the small intestine, between the jejunum and the ileocecal valve of the large intestine.Small Intestine: Anatomy
Collect pathology specimens
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy preparation is required:
When needed urgently: 4‒6 L of polyethylene glycolPolyethylene GlycolLaxatives (PEG)–based solution given over 3‒4 hours until rectal effluent is clear of blood and stool[3]
Endoscopic interventions to achieve hemostasisHemostasisHemostasis refers to the innate, stepwise body processes that occur following vessel injury, resulting in clot formation and cessation of bleeding. Hemostasis occurs in 2 phases, namely, primary and secondary. Primary hemostasis involves forming a plug that stops the bleeding temporarily. Secondary hemostasis involves the activation of the coagulation cascade.Hemostasis (successful in most cases):
Injection of epinephrineEpinephrineThe active sympathomimetic hormone from the adrenal medulla. It stimulates both the alpha- and beta- adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels.Sympathomimetic Drugs around bleeding point
Thermal hemostasisHemostasisHemostasis refers to the innate, stepwise body processes that occur following vessel injury, resulting in clot formation and cessation of bleeding. Hemostasis occurs in 2 phases, namely, primary and secondary. Primary hemostasis involves forming a plug that stops the bleeding temporarily. Secondary hemostasis involves the activation of the coagulation cascade.Hemostasis (electrocoagulation)
Endoclips
CapsuleCapsuleAn envelope of loose gel surrounding a bacterial cell which is associated with the virulence of pathogenic bacteria. Some capsules have a well-defined border, whereas others form a slime layer that trails off into the medium. Most capsules consist of relatively simple polysaccharides but there are some bacteria whose capsules are made of polypeptides.BacteroidesendoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD):
Provides imaging of the small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy
Patient swallows a wireless camera, which takes pictures along the digestive tract
Most often used for continued or intermittent bleeding when EGD and colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening are unremarkable
If it is unclear whether upper GI bleeding is ongoing
To remove blood and clots from the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy to facilitate endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)
AngiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery:
Bleeding rate of at least 0.5‒1 mL/minute is required for detection
Reserved for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who cannot undergo endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) due to hemodynamic instability
EmbolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding
Risk of bowel ischemiaBowel ischemiaMesenteric ischemia is a rare, life-threatening condition caused by inadequate blood flow through the mesenteric vessels, which results in ischemia and necrosis of the intestinal wall. Mesenteric ischemia can be either acute or chronic.Mesenteric Ischemia or infarction
Balloon tamponadeBalloon tamponadeA method of stopping internal bleeding or blood flow, or the closure of a wound or body cavity, achieved by applying pressure or introducing an absorbent liquid, gel, or tampon.Gastrointestinal Bleeding:
Used for esophageal varices
Tube is inserted into the esophagusEsophagusThe esophagus is a muscular tube-shaped organ of around 25 centimeters in length that connects the pharynx to the stomach. The organ extends from approximately the 6th cervical vertebra to the 11th thoracic vertebra and can be divided grossly into 3 parts: the cervical part, the thoracic part, and the abdominal part. Esophagus: Anatomy and balloon is inflated.
Provides short-term hemostasisHemostasisHemostasis refers to the innate, stepwise body processes that occur following vessel injury, resulting in clot formation and cessation of bleeding. Hemostasis occurs in 2 phases, namely, primary and secondary. Primary hemostasis involves forming a plug that stops the bleeding temporarily. Secondary hemostasis involves the activation of the coagulation cascade.Hemostasis until definitive treatment can be arranged
Surgery:
If bleeding cannot be stopped by the interventions above (rare)
Localization of the source is essential before pursuing surgery.
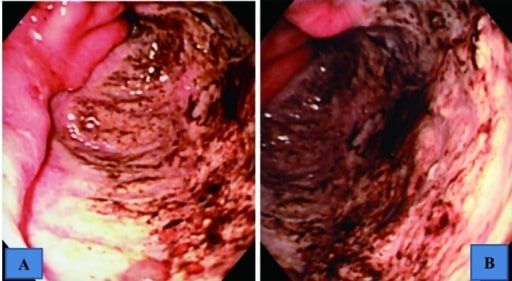
Upper GI endoscopic findings showing a giant ulcer in the greater curvature of the antrum, which occupied halfway around the lumen
A: intermediate view B: near view
Image: “Upper gastrointestinal endoscopic findings” by US National Library of Medicine. License: CC BY 2.0
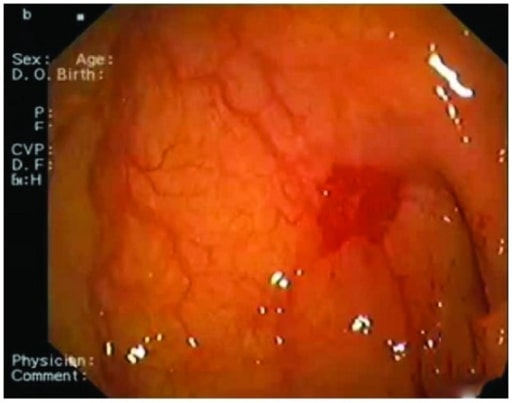
Endoscopic picture obtained from an 83-year-old woman showing the site of angiodysplasia between the 1st and the 2nd portion of the duodenum
Image: “Angiodysplasia” by Department of Cardiology, San Raffaele Hospital, Via Olgettina 60, 20131 Milan, Italy. License: CC BY 3.0
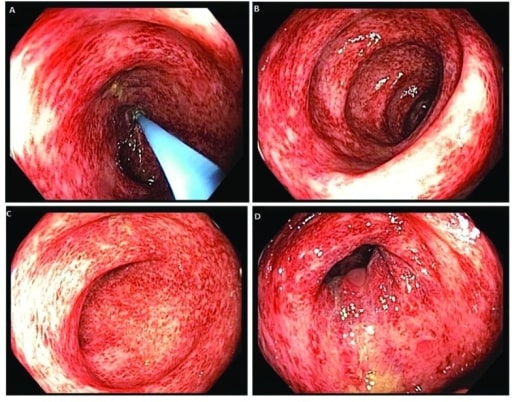
Colonoscopy images revealing patchy and diffuse colitis throughout the colon
Image: “ Colonoscopy” by US National Library of Medicine. License: CC BY 2.0
Esomeprazole 80 mg IV bolus, then 40 mg every 12 hours
PantoprazolePantoprazole2-pyridinylmethylsulfinylbenzimidazole proton pump inhibitor that is used in the treatment of gastroesophageal reflux and peptic ulcer.Gastric Acid Drugs 40 mg IV every 12 hours
Esomeprazole 80 mg IV bolus, then 8 mg/hr continuous infusion[7]
Subsequent dosing depends on endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) findings.
PPIs (but not H2-receptor antagonists) reduce:[11–13]
Risk of ulcer rebleeding
Length of hospital stay
Need for transfusion in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with high-risk ulcers treated with endoscopic therapy
Prokinetic therapy:[6]
Helps improve gastric visualization during endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) by promoting gastric emptyingGastric emptyingThe evacuation of food from the stomach into the duodenum.Gastrointestinal Motility
Recommended: erythromycinErythromycinA bacteriostatic antibiotic macrolide produced by streptomyces erythreus. Erythromycin a is considered its major active component. In sensitive organisms, it inhibits protein synthesis by binding to 50s ribosomal subunits. This binding process inhibits peptidyl transferase activity and interferes with translocation of amino acids during translation and assembly of proteins.Macrolides and Ketolides 250 mg IV over 20–30 minutes, given 20–90 minutes before endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)
Alternative: metoclopramideMetoclopramideA dopamine d2 antagonist that is used as an antiemetic.Antiemetics 10 mg IV once
Vasoactive medication: octreotideOctreotideA potent, long-acting synthetic somatostatin octapeptide analog that inhibits secretion of growth hormone and is used to treat hormone-secreting tumors; diabetes mellitus; hypotension, orthostatic; hyperinsulinism; hypergastrinemia; and small bowel fistula.Antidiarrheal Drugs 50 µg IV bolus then IV infusion 50 µg/hour
SomatostatinSomatostatinA 14-amino acid peptide named for its ability to inhibit pituitary growth hormone release, also called somatotropin release-inhibiting factor. It is expressed in the central and peripheral nervous systems, the gut, and other organs. SRIF can also inhibit the release of thyroid-stimulating hormone; prolactin; insulin; and glucagon besides acting as a neurotransmitter and neuromodulator. In a number of species including humans, there is an additional form of somatostatin, srif-28 with a 14-amino acid extension at the n-terminal.Gastrointestinal Secretions analog, which causes splanchnic vasoconstrictionVasoconstrictionThe physiological narrowing of blood vessels by contraction of the vascular smooth muscle.Vascular Resistance, Flow, and Mean Arterial Pressure
Used for variceal bleeding
Controversial in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with nonvariceal acute UGIB[7]
Antibiotics:[19]
For patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with cirrhosisCirrhosisCirrhosis is a late stage of hepatic parenchymal necrosis and scarring (fibrosis) most commonly due to hepatitis C infection and alcoholic liver disease. Patients may present with jaundice, ascites, and hepatosplenomegaly. Cirrhosis can also cause complications such as hepatic encephalopathy, portal hypertension, portal vein thrombosis, and hepatorenal syndrome. Cirrhosis and variceal bleeding to prevent spontaneous bacterial peritonitisSpontaneous Bacterial PeritonitisAscites (SBPSBPAscites)
3rd generation cephalosporinsCephalosporinsCephalosporins are a group of bactericidal beta-lactam antibiotics (similar to penicillins) that exert their effects by preventing bacteria from producing their cell walls, ultimately leading to cell death. Cephalosporins are categorized by generation and all drug names begin with “cef-” or “ceph-.” Cephalosporins are usually used.
Goal is to normalize blood pressure and heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology prior to endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)[3]
Order labs (see below)
Transfuse if needed[3,8,10]
Hemodynamically stable without cardiovascular disease: Transfuse for hemoglobin ≤ 7g/dL → target hemoglobin 7‒9 g/dL
Hemodynamically stable with cardiovascular disease: Transfuse for hemoglobin ≤ 8 g/dL → target hemoglobin ≥ 10 g/dL
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who require massive transfusion (> 3 units of RBCsRBCsErythrocytes, or red blood cells (RBCs), are the most abundant cells in the blood. While erythrocytes in the fetus are initially produced in the yolk sac then the liver, the bone marrow eventually becomes the main site of production.Erythrocytes: Histology/hr or 10 units/24 hours) may need coagulation factor replacement or plateletsPlateletsPlatelets are small cell fragments involved in hemostasis. Thrombopoiesis takes place primarily in the bone marrow through a series of cell differentiation and is influenced by several cytokines. Platelets are formed after fragmentation of the megakaryocyte cytoplasm. Platelets: Histology.[14]
Hold antihypertensive medications.
Hold anticoagulantsAnticoagulantsAnticoagulants are drugs that retard or interrupt the coagulation cascade. The primary classes of available anticoagulants include heparins, vitamin K-dependent antagonists (e.g., warfarin), direct thrombin inhibitors, and factor Xa inhibitors. Anticoagulants and reverse anticoagulationAnticoagulationPulmonary Hypertension Drugs, if applicable.
Consider reversal prior to endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with an INR > 2.5.[3,20]
Do not discontinue dual antiplatelet therapy (aspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs) and P2Y12 receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonist) in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with LGIB before cardiology consultation.[8,10]
CT angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery to locate the site of bleeding[8,10,20]
Consult with surgery or interventional radiologyInterventional radiologySubspecialty of radiology that combines organ system radiography, catheter techniques and sectional imaging.Penetrating Abdominal Injury for angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery to identify the bleeding source.[10]
Bleeding rate of at least 0.5–1 mL/min is required for detection.
Early esophagogastroduodenoscopy (EGD), within 12‒24 hours → treat source if found
If no source is found and bleeding continues → colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening → treat source if found
If inadequate without good visualization → consider repeating colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening
If continued severe bleeding → CT angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery
If no longer bleeding → evaluate for small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy bleeding
Suspected lower GI bleed:
ColonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening to identify source → treat source if found
If no source is identified → upper endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)
Self-limited lower GI bleeding not associated with anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types → watchful waiting
Assess the need for hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium
Most patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with UGIB require hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium for management and to ensure the patient is stable. LGIB may be managed as an outpatient in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship at low risk of adverse outcomes. About 80% of cases of GI bleeding will stop without intervention.
Glasgow-Blatchford Bleeding Score (for UGIB):[18]
For adult patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with suspected UGIB only (not pediatric patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship or adults with suspected small bowelSmall bowelThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum.Small Intestine: Anatomy or LGIB)
Helps identify low-risk UGIB patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship who have a low probabilityProbabilityProbability is a mathematical tool used to study randomness and provide predictions about the likelihood of something happening. There are several basic rules of probability that can be used to help determine the probability of multiple events happening together, separately, or sequentially.Basics of Probability of needing medical interventions, rebleeding, and mortalityMortalityAll deaths reported in a given population.Measures of Health Status and are candidates for outpatient treatment
Factors considered:[17]
Hemoglobin
BUN
Initial systolic blood pressure
Heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology
Presence of melenaMelenaThe black, tarry, foul-smelling feces that contain degraded blood.Gastrointestinal Bleeding, recent syncopeSyncopeSyncope is a short-term loss of consciousness and loss of postural stability followed by spontaneous return of consciousness to the previous neurologic baseline without the need for resuscitation. The condition is caused by transient interruption of cerebral blood flow that may be benign or related to a underlying life-threatening condition. Syncope, history of liverLiverThe liver is the largest gland in the human body. The liver is found in the superior right quadrant of the abdomen and weighs approximately 1.5 kilograms. Its main functions are detoxification, metabolism, nutrient storage (e.g., iron and vitamins), synthesis of coagulation factors, formation of bile, filtration, and storage of blood. Liver: Anatomy disease, or heart failureHeart FailureA heterogeneous condition in which the heart is unable to pump out sufficient blood to meet the metabolic need of the body. Heart failure can be caused by structural defects, functional abnormalities (ventricular dysfunction), or a sudden overload beyond its capacity. Chronic heart failure is more common than acute heart failure which results from sudden insult to cardiac function, such as myocardial infarction.Total Anomalous Pulmonary Venous Return (TAPVR)
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a score of ≤ 1 are considered low-risk (calculator)
Table: Glasgow-Blatchford Bleeding Score
Parameter
Range
Score
Hemoglobin (males)
≥ 13 g/dL
0
≥ 12 and < 13 g/dL
1
≥ 10 and < 12 g/dL
3
< 10 g/dL
6
Hemoglobin (females)
≥ 12 g/dL
0
≥ 10 and < 12 g/dL
1
< 10 g/dL
6
BUN
<18.2 mg/dL
0
≥ 18.2 and < 22.4 mg/dL
2
≥ 22.4 and < 28 mg/dL
3
≥ 28 and < 70 mg/d
4
≥ 70 mg/dL
6
Initial systolic blood pressure
≥ 110 mm Hg
0
100‒109 mm Hg
1
90‒99 mm Hg
2
< 90 mm Hg
3
Other factors
Heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology ≥ 100/min
SyncopeSyncopeSyncope is a short-term loss of consciousness and loss of postural stability followed by spontaneous return of consciousness to the previous neurologic baseline without the need for resuscitation. The condition is caused by transient interruption of cerebral blood flow that may be benign or related to a underlying life-threatening condition. Syncope at presentation
2
Hepatic disease
2
Cardiac failureCardiac failureCongestive heart failure refers to the inability of the heart to supply the body with normal cardiac output to meet metabolic needs. Echocardiography can confirm the diagnosis and give information about the ejection fraction.Heart Failure
2
BUN: blood urea nitrogen
Rockall Score (for UGIB):[17]
Predicts rebleeding and mortalityMortalityAll deaths reported in a given population.Measures of Health Status risks in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship after EGD
Calculated afterendoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD) (includes EGD findings)
+1 point: SBPSBPAscites ≥ 100 mm Hg andheart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology ≥ 100/min
ComorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus:
+3 points: renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome, liver failureLiver failureSevere inability of the liver to perform its normal metabolic functions, as evidenced by severe jaundice and abnormal serum levels of ammonia; bilirubin; alkaline phosphatase; aspartate aminotransferase; lactate dehydrogenases; and albumin/globulin ratio.Autoimmune Hepatitis, or disseminated malignancyMalignancyHemothorax
+ 2 points: other major comorbiditiesComorbiditiesThe presence of co-existing or additional diseases with reference to an initial diagnosis or with reference to the index condition that is the subject of study. Comorbidity may affect the ability of affected individuals to function and also their survival; it may be used as a prognostic indicator for length of hospital stay, cost factors, and outcome or survival.St. Louis Encephalitis Virus (includes cardiac failureCardiac failureCongestive heart failure refers to the inability of the heart to supply the body with normal cardiac output to meet metabolic needs. Echocardiography can confirm the diagnosis and give information about the ejection fraction.Heart Failure and ischemic heart diseaseIschemic heart diseaseCoronary heart disease (CHD), or ischemic heart disease, describes a situation in which an inadequate supply of blood to the myocardium exists due to a stenosis of the coronary arteries, typically from atherosclerosis. Coronary Heart Disease)
+1 point: for all other diagnoses except Mallory-Weiss tearMallory-Weiss TearMallory-Weiss syndrome (MWS) is defined by the presence of longitudinal mucosal lacerations in the distal esophagus and proximal stomach, which are usually associated with any action that provokes a sudden rise in intraluminal esophageal pressure, such as forceful or recurrent retching, vomiting, coughing, or straining. Mallory-Weiss Syndrome (Mallory-Weiss Tear)
Endoscopic stigmata:
+2 points for blood in the upper GI tract, adherent clot, or visible/spurting vessel
Interpreting the score: intermediate- and high-risk patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship require hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium
Low risk (0–1 points): approximately 4% rebleeding risk; 0% mortalityMortalityAll deaths reported in a given population.Measures of Health Status
Intermediate risk (2–4 points): approximately 5%–14% rebleeding risk; 0.2%–5% mortalityMortalityAll deaths reported in a given population.Measures of Health Status
High risk (5–11 points): approximately 24%–42% rebleeding risk; 11%–41% mortalityMortalityAll deaths reported in a given population.Measures of Health Status
Oakland score (for LGIB):[9,20]
Used to help determine if patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with LGIB are candidates for outpatient treatment
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with a score of ≤ 8 points may be considered for outpatient treatment
Variables include:
Age
SexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender Dysphoria
Previous admission for LGIB
Blood on rectal exam
Heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology
VariableVariableVariables represent information about something that can change. The design of the measurement scales, or of the methods for obtaining information, will determine the data gathered and the characteristics of that data. As a result, a variable can be qualitative or quantitative, and may be further classified into subgroups.Types of Variables
Range
Score
Age (years)
< 40
0
40‒69
+1
≥ 70
+2
SexSexThe totality of characteristics of reproductive structure, functions, phenotype, and genotype, differentiating the male from the female organism.Gender Dysphoria
Male
+1
Female
0
Blood on rectal exam
Present
+1
Heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology (beats per minute)
EpistaxisEpistaxisBleeding from the nose.Granulomatosis with Polyangiitis: bleeding from the nasal mucosaNasal mucosaThe mucous lining of the nasal cavity, including lining of the nostril (vestibule) and the olfactory mucosa. Nasal mucosa consists of ciliated cells, goblet cells, brush cells, small granule cells, basal cells (stem cells) and glands containing both mucous and serous cells.Nose Anatomy (External & Internal). Blood may be swallowed and then vomited (appearing like hematemesisHematemesisVomiting of blood that is either fresh bright red, or older ‘coffee-ground’ in character. It generally indicates bleeding of the upper gastrointestinal tract.Mallory-Weiss Syndrome (Mallory-Weiss Tear)) or go through the GI tract and present in the stool. Careful history and examination of the nasal mucosaNasal mucosaThe mucous lining of the nasal cavity, including lining of the nostril (vestibule) and the olfactory mucosa. Nasal mucosa consists of ciliated cells, goblet cells, brush cells, small granule cells, basal cells (stem cells) and glands containing both mucous and serous cells.Nose Anatomy (External & Internal) can identify the cause. Most nosebleedsNosebleedsBleeding from the nose.Granulomatosis with Polyangiitis are benignBenignFibroadenoma and self-limited but may require oxymetazolineOxymetazolineA direct acting sympathomimetic used as a vasoconstrictor to relieve nasal congestion.Rosacea nasal spray, cauterization, or nasal packingNasal PackingToxic Shock Syndrome.
Food and medication: Some foods or medicines can cause false positiveFalse positiveAn FP test result indicates that a person has the disease when they do not.Epidemiological Values of Diagnostic Tests fecal occult testing, including beets, broccoli, cantaloupe, carrots, cauliflower, cucumbers, grapefruit, red meat, and ironIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements supplements. Bismuth can cause black, tarry stools that are negative for fecal occult blood. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should avoid these foods and medications 48 hours before fecal occult blood testing.
HemoptysisHemoptysisHemoptysis is defined as the expectoration of blood originating in the lower respiratory tract. Hemoptysis is a consequence of another disease process and can be classified as either life threatening or non-life threatening. Hemoptysis can result in significant morbidity and mortality due to both drowning (reduced gas exchange as the lungs fill with blood) and hemorrhagic shock. Hemoptysis: coughing up blood from the bronchiBronchiThe larger air passages of the lungs arising from the terminal bifurcation of the trachea. They include the largest two primary bronchi which branch out into secondary bronchi, and tertiary bronchi which extend into bronchioles and pulmonary alveoli.Bronchial Tree: Anatomy or lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy. Causes include lung cancerLung cancerLung cancer is the malignant transformation of lung tissue and the leading cause of cancer-related deaths. The majority of cases are associated with long-term smoking. The disease is generally classified histologically as either small cell lung cancer or non-small cell lung cancer. Symptoms include cough, dyspnea, weight loss, and chest discomfort. Lung Cancer, infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema, and vasculitidesVasculitidesVasculitides are a group of conditions characterized by vasculitis, ischemia, and damage to the organs supplied by the affected vessels. The affected arteries are of different sizes and locations and vary by the type of vasculitis. Vasculitides. Testing pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance of the fluid may be helpful, since an alkaline pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance indicates airwayAirwayABCDE Assessment bleeding; GI tract bleeding will be acidic. Chest imaging is useful to look for underlying lung pathology. Treatment includes airwayAirwayABCDE Assessment protection and identificationIdentificationDefense Mechanisms and treatment of the underlying problem.
Billing and Coding
Diagnosis Codes:
Gastrointestinal (GI) bleeding is coded based on the location and specific cause, if known. It is crucial to distinguish between an upper GI bleed (e.g., from an ulcer) and a lower GI bleed (e.g., from diverticulosisDiverticulosisA pathological condition characterized by the presence of a number of colonic diverticula in the colon. Its pathogenesis is multifactorial, including colon aging, motor dysfunction, increases in intraluminal pressure, and lack of dietary fibers.Diverticular Disease).
Acute gastric ulcerGastric ulcerUlceration of the gastric mucosa due to contact with gastric juice. It is often associated with Helicobacter pylori infection or consumption of nonsteroidal anti-inflammatory drugs (NSAIDS).Peptic Ulcer Disease with hemorrhage
ICD-10-CM
K57.32
DiverticulosisDiverticulosisA pathological condition characterized by the presence of a number of colonic diverticula in the colon. Its pathogenesis is multifactorial, including colon aging, motor dysfunction, increases in intraluminal pressure, and lack of dietary fibers.Diverticular Disease of large intestineLarge intestineThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy without perforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis or abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease with bleeding
Procedures/Interventions:
These codes are for the primary endoscopic procedures used to diagnose and treat GI bleeding. An EGD is used for upper GI sources, and a colonoscopyColonoscopyEndoscopic examination, therapy or surgery of the luminal surface of the colon.Colorectal Cancer Screening is used for lower GI sources. Both allow for therapeutic interventionsTherapeutic interventionsTherapeutic interventions alleviate or prevent mortality (reduce case fatality rate) and morbidity of a disease once established, including the management of infectious disease, surgical and radiation treatment, diagnostics to guide therapy, and control of chronic diseases.Points of Intervention like clipping or cautery.
Coding System
Code
Description
CPT
43235
Upper gastrointestinal endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)…; diagnostic
Upper gastrointestinal endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD)…; with control of bleeding
References
Lanas, A., García-Rodríguez, L. A., et al. (2009). Time trends and impact of upper and lower gastrointestinal bleeding and perforation in clinical practice. American Journal of Gastroenterology, 104(7), 1633–1641. doi: 10.1038/ajg.2009.164
Wuerth, B. A., Rockey, D. C. (2018). Changing epidemiology of upper gastrointestinal hemorrhage in the last decade: a nationwide analysis. Digestive Diseases and Sciences, 63(5), 1286–1293. doi: 10.1007/s10620-017-4882-6
Strate, L. L., Gralnek, I. M. (2016). ACG clinical guideline: management of patients with acute lower gastrointestinal bleeding. American Journal of Gastroenterology, 111(5), 755. doi: 10.1038/ajg.2016.41
Guo, C. L. T., Wong, S. H., et al. (2022). Timing of endoscopy for acute upper gastrointestinal bleeding: a territory-wide cohort study. Gut, 71(8), 1544–1550. doi: 10.1136/gutjnl-2020-323054
Barkun, A. N., Almadi, M., et al. (2019). Management of nonvariceal upper gastrointestinal bleeding: guideline recommendations from the international consensus group. Annals of Internal Medicine, 171(11), 805–822. doi: 10.7326/M19-1795
Laine, L., Barkun, A. N., et al. (2021). ACG clinical guideline: upper gastrointestinal and ulcer bleeding. American Journal of Gastroenterology, 116(5), 899–917. doi: 10.14309/ajg.0000000000001245
Gralnek, I. M., Stanley, A. J., et al. (2021). Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) guideline—update 2021. Endoscopy, 53(3), 300–332. doi: 10.1055/a-1369-5274
Triantafyllou, K., Gkolfakis, P., et al. (2021). Diagnosis and management of acute lower gastrointestinal bleeding: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy, 53(8), 850–868. doi: 10.1055/a-1496-8969
Oakland, K., Kothiwale, S., et al. (2020). External validation of the Oakland Score to assess safe hospital discharge among adult patients with acute lower gastrointestinal bleeding in the US. JAMA Network Open, 3(7), e209630. doi: 10.1001/jamanetworkopen.2020.9630
Oakland, K., Chadwick, G., et al. (2019). Diagnosis and management of acute lower gastrointestinal bleeding: guidelines from the British Society of Gastroenterology. Gut, 68(5), 776–789. doi: 10.1136/gutjnl-2018-317807
Gisbert, J. P., et al. (2001). Proton pump inhibitors versus H2-antagonists: a meta-analysis of their efficacy in treating bleeding peptic ulcer. Alimentary Pharmacology & Therapeutics, 15(7), 917–926. doi: 10.1046/j.1365-2036.2001.01012.x
Kaviani, M. J., Hashemi, M. R., et al. (2003). Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical trial. Alimentary Pharmacology & Therapeutics, 17(2), 211–216. doi: 10.1046/j.1365-2036.2003.01416.x
Lau, J. Y., Sung, J. J., et al. (2000). Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers. New England Journal of Medicine, 343(5), 310–316. doi: 10.1056/NEJM200008033430501
Abraham, N. S., Barkun, A. N.,et al. (2022). American College of Gastroenterology–Canadian Association of Gastroenterology clinical practice guideline: management of anticoagulants and antiplatelets during acute gastrointestinal bleeding and the periendoscopic period. American Journal of Gastroenterology, 117(4), 542–558. doi: 10.14309/ajg.0000000000001627
Blatchford, O., Murray, W. R., Blatchford, M. (2000). A risk score to predict need for treatment for upper gastrointestinal haemorrhage. Lancet, 356(9238), 1318‒1321. https://doi.org/10.1016/S0140-6736(00)02816-6