Chronic pancreatitis (CP) is due to persistent inflammation, fibrosis, and irreversible cell damage to the pancreas, resulting in a loss of endocrine and exocrine gland function. Irreversible damage distinguishes CP from acute pancreatitis, in which the damage is reversible. The most common etiologies are alcohol abuse and pancreatic duct obstruction, and there is a strong association with cigarette smoking. Patients often present with recurrent epigastric abdominal pain, nausea, and features of malabsorption syndrome (diarrhea, steatorrhea, and weight loss). Characteristic computed tomography (CT) findings depend on the severity and range from mild ductal dilatation and gland enlargement to severe ductal dilatation, large cavity formations, and calcifications. Therapy focuses on alcohol cessation, diet changes, pain management, and treatment of pancreatic insufficiency. Endoscopic or surgical decompression of large ducts may be necessary, and patients who have intractable pain with small duct disease may require pancreatic resection.
Epidemiologic data are limited due to varying diagnostic criteria for the disease.
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 5–12 per 100,000 people
Alcohol-relateddisease more common in Western countries and Japan:
Associated with over half of all cases in the United States
< 5% of heavy drinkers develop chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Potential cofactors include diet, genetic background, ancestry, type of alcohol, and smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases.
Common etiologies of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis are summarized with the “TIGAR-O” mnemonic:
Table: TIGAR-O: Common etiologies of pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
T
Toxic/metabolic
Alcohol (most common)
Tobacco smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
HypercalcemiaHypercalcemiaHypercalcemia (serum calcium > 10.5 mg/dL) can result from various conditions, the majority of which are due to hyperparathyroidism and malignancy. Other causes include disorders leading to vitamin D elevation, granulomatous diseases, and the use of certain pharmacological agents. Symptoms vary depending on calcium levels and the onset of hypercalcemia. Hypercalcemia
Autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance: PRSS1
Autosomal recessiveAutosomal recessiveAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal recessive diseases are only expressed when 2 copies of the recessive allele are inherited.Autosomal Recessive and Autosomal Dominant Inheritance:
CFTR
SPINK1
A
Autoimmune
Autoimmune pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitistype 1Type 1Spinal Muscular Atrophy: immunoglobulin G4 (IgG4)–related disease
Autoimmune pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis type 2: idiopathicIdiopathicDermatomyositis duct centric pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
R
Recurrent acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
The strongest risk factor for developing chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
CFTR: cysticCysticFibrocystic ChangefibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans is most common cause in children
GeneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics abbreviations:
PRSS1 → cationic trypsinogenTrypsinogenThe inactive proenzyme of trypsin secreted by the pancreas, activated in the duodenum via cleavage by enteropeptidase.Pancreatic Parameters:
Gain-of-function mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations resulting in abnormal trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides
Activates digestive enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes in the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
Leads to ongoing damage
CFTR → cysticCysticFibrocystic ChangefibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans transmembrane conductance regulator geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics:
Modifier geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics that increases susceptibility to chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis and accelerates progression
Multiple types of mutations result in different effects on exocrine function
SPINK1 → pancreatic secretory trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides inhibitor geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics:
Responsible for inhibiting prematurely activated intra-pancreatic trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides
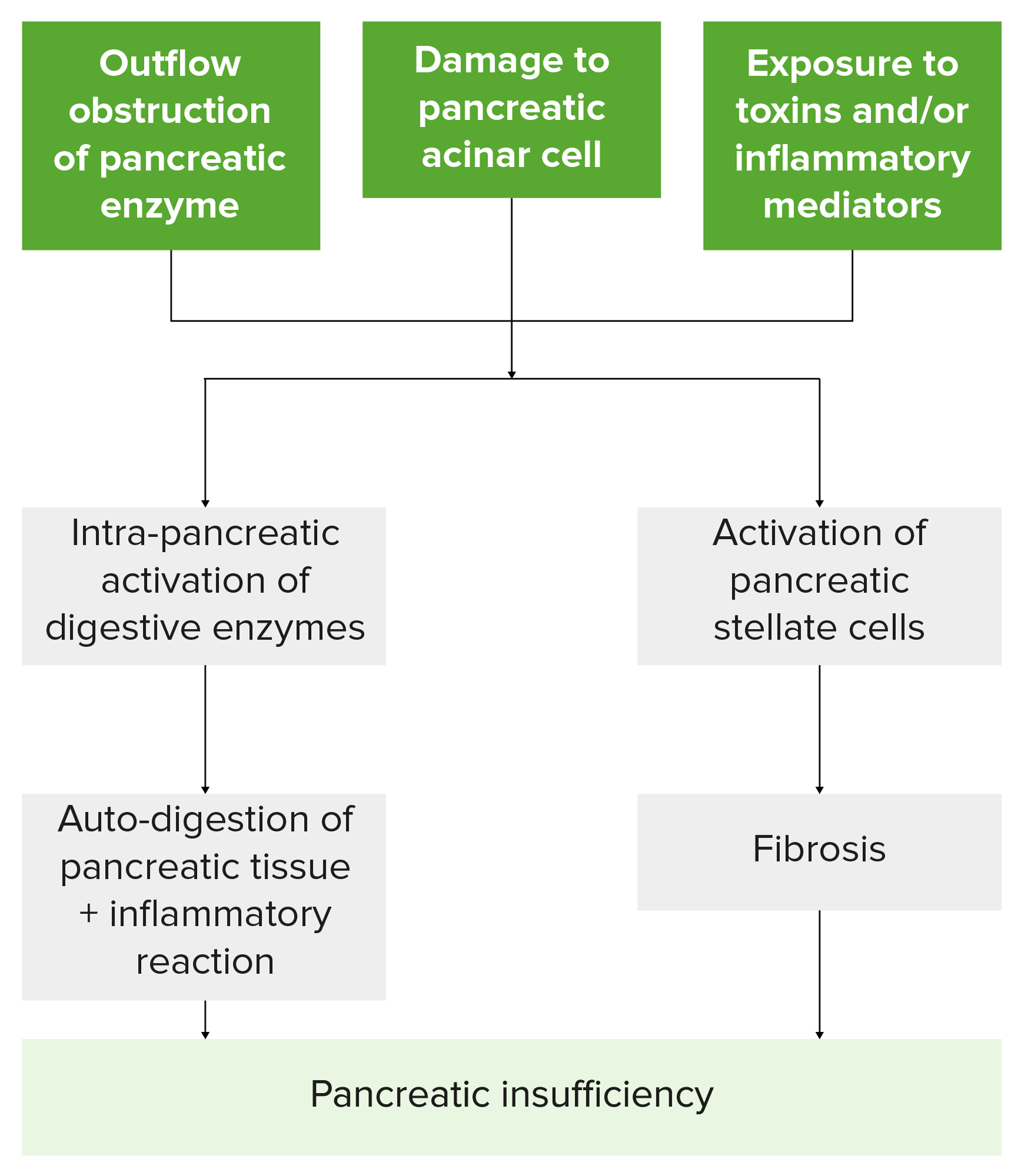
After the cells are injured by one of the “TIGAR-O” causes, the “sentinel acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis event (SAPE)” hypothesisHypothesisA hypothesis is a preliminary answer to a research question (i.e., a “guess” about what the results will be). There are 2 types of hypotheses: the null hypothesis and the alternative hypothesis.Statistical Tests and Data Representation uniformly describes the pathogenesis of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, as follows:
Episode of acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis (AP) alters the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy to make it hypersensitive to recurrent AP.
Initially, there is matrix metalloproteinase-mediated destruction of normal collagenCollagenA polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth).Connective Tissue: Histology and activation of pancreatic stellate cellsStellate cellsCerebellum: Anatomy (PSCs, also called periacinar myofibroblastsMyofibroblastsSpindle-shaped cells with characteristic contractile proteins and structures that contribute to the wound healing process. They occur in granulation tissue and also in pathological processes such as fibrosis.Hypertrophic and Keloid Scars).
PSCs proliferate and synthesize new collagenCollagenA polypeptide substance comprising about one third of the total protein in mammalian organisms. It is the main constituent of skin; connective tissue; and the organic substance of bones (bone and bones) and teeth (tooth).Connective Tissue: Histology with extracellular matrixExtracellular matrixA meshwork-like substance found within the extracellular space and in association with the basement membrane of the cell surface. It promotes cellular proliferation and provides a supporting structure to which cells or cell lysates in culture dishes adhere.Hypertrophic and Keloid Scars (ECM) remodeling.
PSCPSCPrimary sclerosing cholangitis (PSC) is an inflammatory disease that causes fibrosis and strictures of the bile ducts. The exact etiology is unknown, but there is a strong association with IBD. Patients typically present with an insidious onset of fatigue, pruritus, and jaundice, which can progress to cirrhosis and complications related to biliary obstruction. Primary Sclerosing Cholangitis activity is induced by proinflammatory cytokinesProinflammatory CytokinesMetabolic Syndrome, TNF-ɑ, IL-1, IL-6, PSGF, and oxidant complexes.
PSCPSCPrimary sclerosing cholangitis (PSC) is an inflammatory disease that causes fibrosis and strictures of the bile ducts. The exact etiology is unknown, but there is a strong association with IBD. Patients typically present with an insidious onset of fatigue, pruritus, and jaundice, which can progress to cirrhosis and complications related to biliary obstruction. Primary Sclerosing Cholangitis activation may explain disease progression even after removal of noxious stimuli, through a TGF-β-mediated pathway.
FibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans
Progressive atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation (destruction of both exocrine and endocrine tissue)
Pancreatic damage leads to:[1,4–6]
Calcifications
Exocrine insufficiency:
Decreased lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion, amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption, and proteaseProteaseEnzyme of the human immunodeficiency virus that is required for post-translational cleavage of gag and gag-pol precursor polyproteins into functional products needed for viral assembly. HIV protease is an aspartic protease encoded by the amino terminus of the pol gene.HIV Infection and AIDS
Results in malabsorptionMalabsorptionGeneral term for a group of malnutrition syndromes caused by failure of normal intestinal absorption of nutrients.Malabsorption and Maldigestion and maldigestionMaldigestionMalabsorption involves many disorders in which there is an inability of the gut to absorb nutrients from dietary intake, potentially including water and/or electrolytes. A closely related term, maldigestion is the inability to break down large molecules of food into their smaller constituents. Malabsorption and maldigestion can affect macronutrients (fats, proteins, and carbohydrates), micronutrients (vitamins and minerals), or both. Malabsorption and Maldigestion
Endocrine insufficiency:
Destruction of β cells
Results in decreased insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin production
Flowchart summarizing how insults to the pancreas lead to pancreatic insufficiency. Note that injury leads to the activation of pancreatic stellate cells and digestive enzymes, resulting in damaged pancreatic tissue, inflammation, fibrosis, and the loss of exocrine and endocrine cell function.
Does not necessarily correlate with the severity of changes on imaging
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
SteatorrheaSteatorrheaA condition that is characterized by chronic fatty diarrhea, a result of abnormal digestion and/or intestinal absorption of fats.Diarrhea:
Oily, foul-smelling, and floating stools
Due to maldigestionMaldigestionMalabsorption involves many disorders in which there is an inability of the gut to absorb nutrients from dietary intake, potentially including water and/or electrolytes. A closely related term, maldigestion is the inability to break down large molecules of food into their smaller constituents. Malabsorption and maldigestion can affect macronutrients (fats, proteins, and carbohydrates), micronutrients (vitamins and minerals), or both. Malabsorption and Maldigestion of fat
Weight lossWeight lossDecrease in existing body weight.Bariatric Surgery (due to steatorrheaSteatorrheaA condition that is characterized by chronic fatty diarrhea, a result of abnormal digestion and/or intestinal absorption of fats.Diarrhea or fear of eating due to painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways)
Rarely, patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may be asymptomatic.
Physical exam[2,4,6]
Signs of malnutritionMalnutritionMalnutrition is a clinical state caused by an imbalance or deficiency of calories and/or micronutrients and macronutrients. The 2 main manifestations of acute severe malnutrition are marasmus (total caloric insufficiency) and kwashiorkor (protein malnutrition with characteristic edema).Malnutrition in children in resource-limited countries:
The diagnosis of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis relies on a combination of clinical history, physical examination, and imaging. The following information is based on US, UK, and European guidelines.
Imaging
Contrast-enhanced abdominal computed tomography (CT) or magnetic resonance imaging (MRI):[6–9,11,13,15]
Best initial tests
Findings:
Parenchymal and intraductal calcifications
Pancreatic atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation
Dilated pancreatic ducts
Low sensitivity in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with early or mild disease
Helpful in:
Diagnosing complications related to chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Ruling out other conditions
Endoscopic ultrasound (EUS):[6–9,11,13,15]
2nd-line: used if CT and MRI are not diagnostic, but there is a high index of suspicion
Can detect early disease
Nonspecific, and changes can be seen in other patient populations
Parenchymal abnormalities:
HyperechoicHyperechoicA structure that produces a high-amplitude echo (lighter grays and white)Ultrasound (Sonography) foci and stranding
Lobular contour
CystsCystsAny fluid-filled closed cavity or sac that is lined by an epithelium. Cysts can be of normal, abnormal, non-neoplastic, or neoplastic tissues.Fibrocystic Change
Secretin-enhanced magnetic resonance cholangiopancreatographyMagnetic resonance cholangiopancreatographyNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis (s-MRCP):[6–9,11,13]
3rd-line: indicated when CT, MRI, and EUS findings are equivocal
More sensitive in detecting early disease than standard cross-sectional imaging
IV secretinSecretinA peptide hormone of about 27 amino acids from the duodenal mucosa that activates pancreatic secretion and lowers the blood sugar level.Gastrointestinal Secretions allows evaluation of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy’s exocrine response.
Findings:
Ductal strictures and dilations giving a “chain of lakes” or “string of pearls” appearance
Pancreatic calcifications
Endoscopic retrograde cholangiopancreatographyEndoscopic Retrograde CholangiopancreatographyFiberoptic endoscopy designed for duodenal observation and cannulation of Vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (Vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis (ERCPERCPFiberoptic endoscopy designed for duodenal observation and cannulation of vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis):[6–12]
Rarely used for diagnosis
Does not evaluate the parenchyma
Invasive and expensive
Often reserved for stone removal and stent placement (pancreatic duct structures)
American Pancreatic Association recommends considering ERCPERCPFiberoptic endoscopy designed for duodenal observation and cannulation of vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis in situations where all other imaging and pancreatic function testsPancreatic Function TestsChronic Pancreatitis are inconclusive.[8]
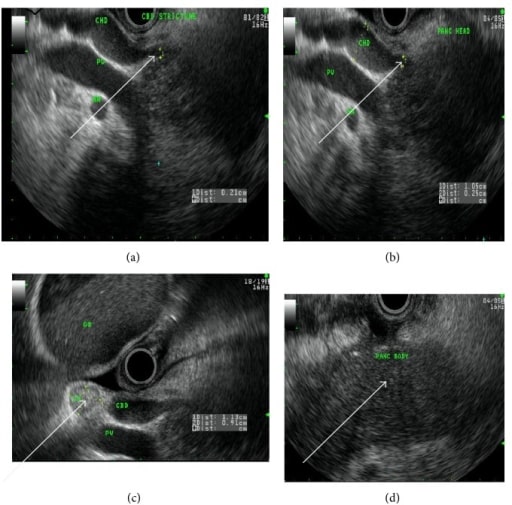
A 50-year-old Caucasian woman with autoimmune chronic pancreatitis. Endoscopic ultrasound image arrows showing (clockwise) (a) common bile duct stricture, (b) dilated common hepatic duct, (c) reactive lymph node, and (d) homogenous pancreatic body.
Image: “fig2” by Lahey Clinic, Burlington, MA 01805, USA. License: CC BY 3.0
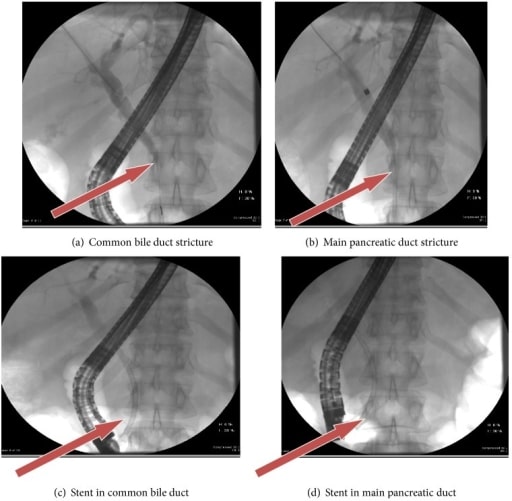
A 50-year-old woman with autoimmune chronic pancreatitis. Arrows in ERCP show common bile duct and main pancreatic duct strictures pre-stent insertion (a and b) and post-stent insertion (c and d).
Image: “fig3” by Lahey Clinic, Burlington, MA 01805, USA. License: CC BY 3.0
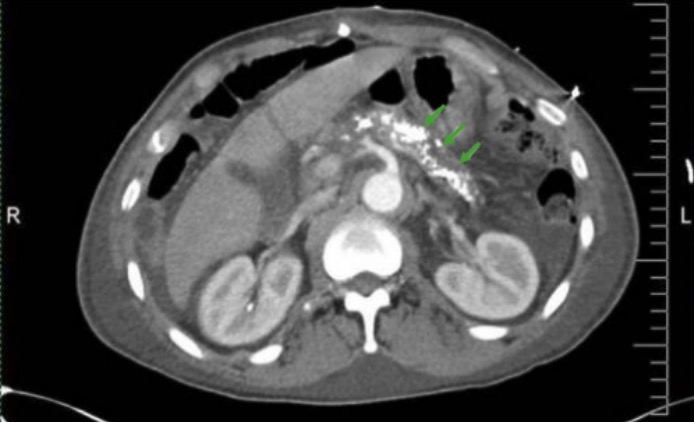
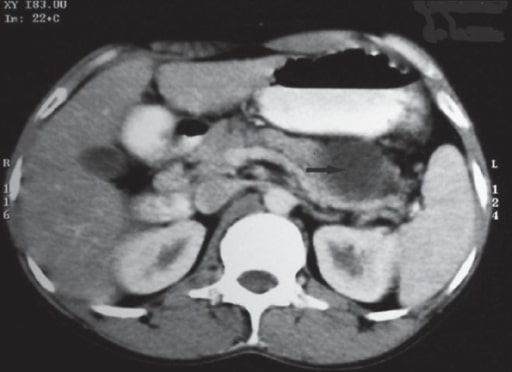
Image: “CT Abdomen” by Division of Gastroenterology and Hepatology, University of Alabama at Birmingham, Birmingham, AL, BDB 380, USA. License: CC BY 3.0
Evaluates for exocrine pancreatic insufficiencyExocrine pancreatic insufficiencyA malabsorption condition resulting from greater than 10% reduction in the secretion of pancreatic digestive enzymes (lipase; proteases; and amylase) by the exocrine pancreas into the duodenum. This condition is often associated with cystic fibrosis and with chronic pancreatitis.Malabsorption and Maldigestion → may be normal in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship without clinically significant insufficiency
Can potentially detect early disease, but more sensitive for late disease
Direct function testing:
Expensive, invasive, and requires a skilled practitioner
Requires fluoroscopyFluoroscopyProduction of an image when x-rays strike a fluorescent screen.X-rays
Exogenous secretinSecretinA peptide hormone of about 27 amino acids from the duodenal mucosa that activates pancreatic secretion and lowers the blood sugar level.Gastrointestinal Secretions and/or cholecystokininCholecystokininA peptide, of about 33 amino acids, secreted by the upper intestinal mucosa and also found in the central nervous system. It causes gallbladder contraction, release of pancreatic exocrine (or digestive) enzymes, and affects other gastrointestinal functions. Cholecystokinin may be the mediator of satiety.Gastrointestinal Secretions are injected → stimulation of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
Duodenal or pancreatic aspirates are measured for:
BicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.Electrolytes
ProteaseProteaseEnzyme of the human immunodeficiency virus that is required for post-translational cleavage of gag and gag-pol precursor polyproteins into functional products needed for viral assembly. HIV protease is an aspartic protease encoded by the amino terminus of the pol gene.HIV Infection and AIDS
AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption
LipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion
Indirect function testing:
Measurements of chymotrypsinChymotrypsinA serine endopeptidase secreted by the pancreas as its zymogen, chymotrypsinogen and carried in the pancreatic juice to the duodenum where it is activated by trypsin. It selectively cleaves aromatic amino acids on the carboxyl side.Pancreatic Parameters and/or elastaseElastaseA protease of broad specificity, obtained from dried pancreas. Molecular weight is approximately 25, 000. The enzyme breaks down elastin, the specific protein of elastic fibers, and digests other proteins such as fibrin, hemoglobin, and albumin.Proteins and Peptides in fecal samples → exocrine insufficiency
Can be used to quantify degree of exocrine insufficiency
Laboratory testing
Laboratory testing is used as an adjunct to imaging.
Blood work:[11,12]
AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption and lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion:
May be elevated, but usually normal in the later stages (due to atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation and fibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy → decreased enzyme production)
No diagnostic value
Liver function testsLiver function testsLiver function tests, also known as hepatic function panels, are one of the most commonly performed screening blood tests. Such tests are also used to detect, evaluate, and monitor acute and chronic liver diseases.Liver Function Tests: ↑ bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism and alkaline phosphataseAlkaline PhosphataseAn enzyme that catalyzes the conversion of an orthophosphoric monoester and water to an alcohol and orthophosphate.Osteosarcoma → suspect pancreatic obstruction
TriglyceridesTriglyceridesFatty Acids and Lipids: fasting level > 1,000 is associated with pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes: to evaluate for hyperparathyroidismHyperparathyroidismHyperparathyroidism is a condition associated with elevated blood levels of parathyroid hormone (PTH). Depending on the pathogenesis of this condition, hyperparathyroidism can be defined as primary, secondary or tertiary. Hyperparathyroidism (rare cause of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis)
Fecal evaluations:[7,12]
↑ 72-hour fecal fat measurement (nonspecific)
↓ Fecal chymotrypsinChymotrypsinA serine endopeptidase secreted by the pancreas as its zymogen, chymotrypsinogen and carried in the pancreatic juice to the duodenum where it is activated by trypsin. It selectively cleaves aromatic amino acids on the carboxyl side.Pancreatic Parameters:
Used in indirect pancreatic function testing
Can also be used for monitoring complianceComplianceDistensibility measure of a chamber such as the lungs (lung compliance) or bladder. Compliance is expressed as a change in volume per unit change in pressure.Veins: Histology with pancreatic enzyme supplementation[8]
↓ Fecal elastaseElastaseA protease of broad specificity, obtained from dried pancreas. Molecular weight is approximately 25, 000. The enzyme breaks down elastin, the specific protein of elastic fibers, and digests other proteins such as fibrin, hemoglobin, and albumin.Proteins and Peptides (used in indirect pancreatic function testing)
Rare diagnostic evaluations:[7,11,12,15]
↑ IgG4 → autoimmune pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis (AIP)
Genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies (for young patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship and those with a strong family historyFamily HistoryAdult Health Maintenance)
European guidelines recommend evaluating for nutritional deficiencies, including:[13]
Prealbumin
Vitamin DVitamin DA vitamin that includes both cholecalciferols and ergocalciferols, which have the common effect of preventing or curing rickets in animals. It can also be viewed as a hormone since it can be formed in skin by action of ultraviolet rays upon the precursors, 7-dehydrocholesterol and ergosterol, and acts on vitamin D receptors to regulate calcium in opposition to parathyroid hormone.Fat-soluble Vitamins and their Deficiencies (25-hydroxycholecalciferol)
IronIronA metallic element with atomic symbol fe, atomic number 26, and atomic weight 55. 85. It is an essential constituent of hemoglobins; cytochromes; and iron-binding proteins. It plays a role in cellular redox reactions and in the transport of oxygen.Trace Elements
ZincZincA metallic element of atomic number 30 and atomic weight 65. 38. It is a necessary trace element in the diet, forming an essential part of many enzymes, and playing an important role in protein synthesis and in cell division. Zinc deficiency is associated with anemia, short stature, hypogonadism, impaired wound healing, and geophagia. It is known by the symbol zn.Trace Elements
MagnesiumMagnesiumA metallic element that has the atomic symbol mg, atomic number 12, and atomic weight 24. 31. It is important for the activity of many enzymes, especially those involved in oxidative phosphorylation.Electrolytes
Fine-needle biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma[7]
Despite being considered the gold standard for diagnosis, biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma and histology evaluation are considered only for cases in which other diagnostic methods have not assisted in establishing a diagnosis.
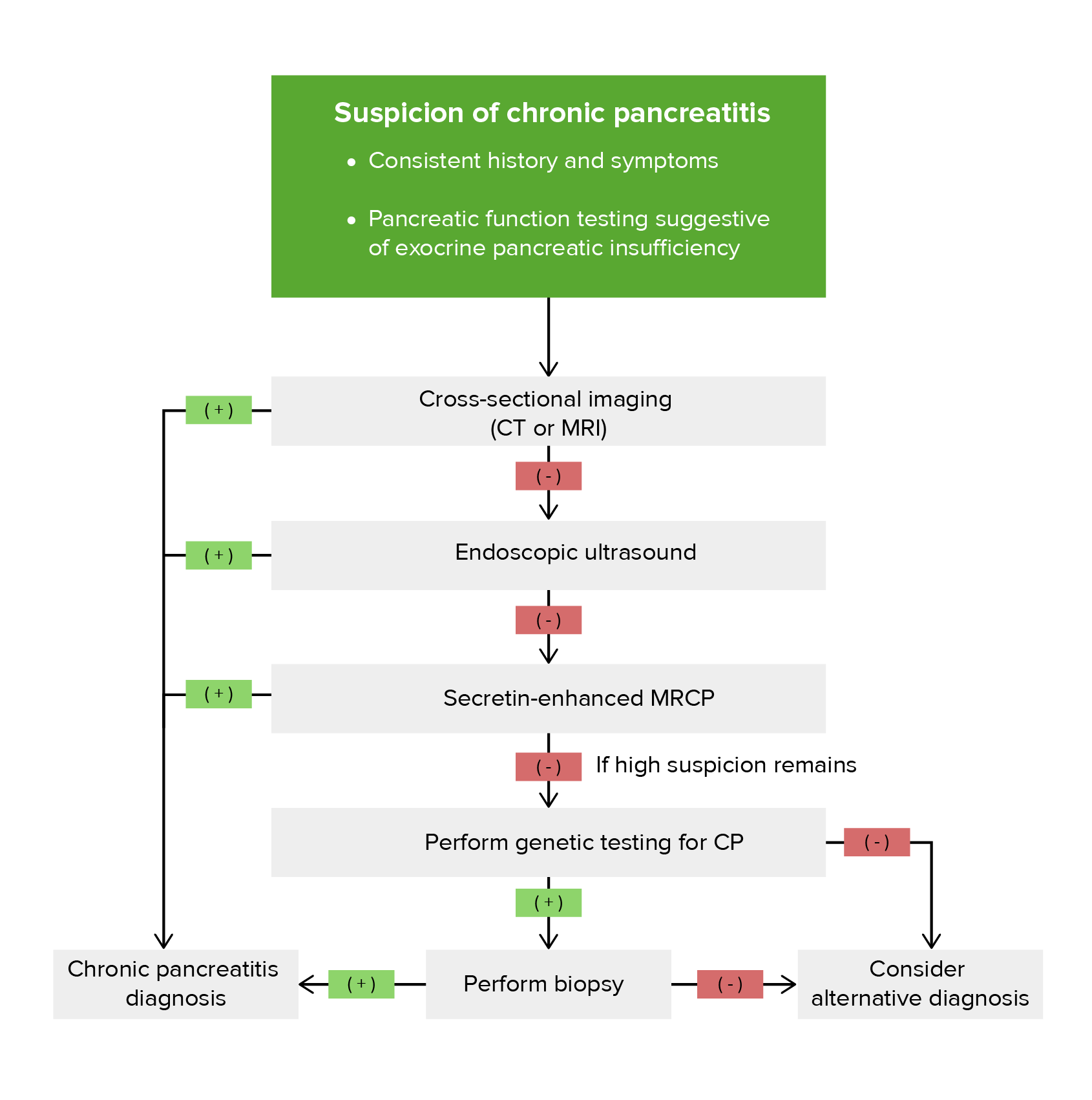
Algorithm for approach to the diagnosis of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis[7,8,11,12]
Diagnostic algorithm for chronic pancreatitis (CP)
Image by Lecturio.
Management
Management protocols may vary based on location. The following recommendations are based on US, UK, and European guidelines.
Lifestyle changes[7–12,15]
Abstinence from alcohol and smokingSmokingWillful or deliberate act of inhaling and exhaling smoke from burning substances or agents held by hand.Interstitial Lung Diseases
Small, frequent, low-fat meals
Adequate hydration
Supplementation of fat-soluble vitamins (A, D, E, K)
Consultants[7,9,11,13]
Management often requires a multidisciplinary approach, including the expertise and assistance of:
Gastroenterology
Endocrinology
Surgery
Specialist pancreatic center
Pancreatic insufficiency management
Endocrine insufficiency:[9,15]
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are at high risk of developing diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus.
Monitor every 6 months for the potential need for insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin therapy.
Exocrine insufficiency:
Pancreatic enzyme replacementEnzyme replacementTherapeutic replacement or supplementation of defective or missing enzymes to alleviate the effects of enzyme deficiency (e.g., glucosylceramidase replacement for gaucher disease).Severe Combined Immunodeficiency (SCID): lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion[7,11,13]
Starting dose: ≥ 40,000‒50,000 USP units with meals[7,13]
A half dose can be given with snacks.[13]
Monitor for improvement in symptoms (e.g., steatorrheaSteatorrheaA condition that is characterized by chronic fatty diarrhea, a result of abnormal digestion and/or intestinal absorption of fats.Diarrhea, weight lossWeight lossDecrease in existing body weight.Bariatric Surgery).
May need to increase dose based on clinical response.
If not responding, can perform pancreatic function testing with oral enzyme administration.[13]
Used in cases where there is inadequate response to enzyme replacementEnzyme replacementTherapeutic replacement or supplementation of defective or missing enzymes to alleviate the effects of enzyme deficiency (e.g., glucosylceramidase replacement for gaucher disease).Severe Combined Immunodeficiency (SCID)
Can improve effect of enzyme replacementEnzyme replacementTherapeutic replacement or supplementation of defective or missing enzymes to alleviate the effects of enzyme deficiency (e.g., glucosylceramidase replacement for gaucher disease).Severe Combined Immunodeficiency (SCID) therapy
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways treatment
Medications:[7,11,12,15]
Nonsteroidal antiinflammatory drugsNonsteroidal Antiinflammatory DrugsNonsteroidal antiinflammatory drugs (NSAIDs) are a class of medications consisting of aspirin, reversible NSAIDs, and selective NSAIDs. NSAIDs are used as antiplatelet, analgesic, antipyretic, and antiinflammatory agents. Nonsteroidal Antiinflammatory Drugs (NSAIDs) (NSAIDsNSAIDSPrimary vs Secondary Headaches) and acetaminophenAcetaminophenAcetaminophen is an over-the-counter nonopioid analgesic and antipyretic medication and the most commonly used analgesic worldwide. Despite the widespread use of acetaminophen, its mechanism of action is not entirely understood.Acetaminophen: 1st-line[11–13]
OpioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics for severe painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways:[7,11‒13]
Consider when other therapeutic options have been exhausted
Weaker agents 1st: tramadolTramadolA narcotic analgesic proposed for severe pain. It may be habituating.Opioid Analgesics
Stronger agents if painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways persists: oxycodoneOxycodoneA semisynthetic derivative of codeine.Opioid Analgesics or morphineMorphineThe principal alkaloid in opium and the prototype opiate analgesic and narcotic. Morphine has widespread effects in the central nervous system and on smooth muscle.Opioid Analgesics
Opt for the lowest effective dose.
Adjuncts:
Low-dose antidepressants (may help with concomitant depression):[12,13]
Tricyclic antidepressantsTricyclic antidepressantsTricyclic antidepressants (TCAs) are a class of medications used in the management of mood disorders, primarily depression. These agents, named after their 3-ring chemical structure, act via reuptake inhibition of neurotransmitters (particularly norepinephrine and serotonin) in the brain.Tricyclic Antidepressants
Combined serotoninSerotoninA biochemical messenger and regulator, synthesized from the essential amino acid l-tryptophan. In humans it is found primarily in the central nervous system, gastrointestinal tract, and blood platelets. Serotonin mediates several important physiological functions including neurotransmission, gastrointestinal motility, hemostasis, and cardiovascular integrity.Receptors and Neurotransmitters of the CNS and norepinephrineNorepinephrinePrecursor of epinephrine that is secreted by the adrenal medulla and is a widespread central and autonomic neurotransmitter. Norepinephrine is the principal transmitter of most postganglionic sympathetic fibers, and of the diffuse projection system in the brain that arises from the locus ceruleus.Receptors and Neurotransmitters of the CNS reuptake inhibitors
GabapentinGabapentinA cyclohexane-gamma-aminobutyric acid derivative that is used for the treatment of partial seizures; neuralgia; and restless legs syndrome.Second-Generation Anticonvulsant Drugs and pregabalinPregabalinA gamma-aminobutyric acid (gaba) derivative that functions as a calcium channel blocker and is used as an anticonvulsant as well as an anti-anxiety agent. It is also used as an analgesic in the treatment of neuropathic pain and fibromyalgia.Second-Generation Anticonvulsant Drugs: target the neuropathic component of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways[9,11,13]
AntioxidantsAntioxidantsNaturally occurring or synthetic substances that inhibit or retard oxidation reactions. They counteract the damaging effects of oxidation in animal tissues.Cell Injury and Death:[7,11,12]
Suggested by American College of Gastroenterology; not recommended by European guidelines
Small effect on painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
Includes vitamins E and C, seleniumSeleniumAn element with the atomic symbol se, atomic number 34, and atomic weight 78. 97. It is an essential micronutrient for mammals and other animals but is toxic in large amounts. Selenium protects intracellular structures against oxidative damage. It is an essential component of glutathione peroxidase.Trace Elements, beta-carotene, and methionine
Pancreatic enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes show limited benefit in treatment of painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and should be reserved for patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with pancreatic exocrine insufficiency.[7,11]
Procedures for intractable painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways:[7,11–14,15]
Celiac plexus blockade (does not result in long-lasting painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways relief)
Endoscopic treatment/ERCPERCPFiberoptic endoscopy designed for duodenal observation and cannulation of vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis for decompression of blocked pancreatic ducts:
Directed to the specific pancreatic duct with obstruction, if present
SphincterotomySphincterotomySurgical incision of a sphincter.Anal Fissure, stone extraction, drainage of pancreatic pseudocystPancreatic pseudocystCyst-like space not lined by epithelium and contained within the pancreas. Pancreatic pseudocysts account for most of the cystic collections in the pancreas and are often associated with chronic pancreatitis.Acute Cholangitis
Stent placement has significant complications, so surgical therapy for ductal decompression is preferred.
Extracorporeal shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock wave lithotripsy of pancreatic stones
FistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula
In some instances, may be preferable to endoscopic procedures
Type of surgery depends on the pancreatic duct anatomy, patient’s history, and complications:
Resection if intractable painful small duct disease
Decompression of large duct obstruction
Autoimmune pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis[8,11,12]
Rule out pancreatic cancer with EUS with fine-needle biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma → can masquerade as AIP
Consider glucocorticoid trial after pancreatic cancer is ruled out.
No response to glucocorticoid in 2‒3 weeks → refer to surgery (Surgical exploration for pancreatic cancer may be warranted.)
Pancreatic cancer risk
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship are at an elevated risk for pancreatic cancer (higher for hereditary chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis).
US:[11]
Routine screeningScreeningPreoperative Care for pancreatic cancer is not recommended unless a PRSS1mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations is present.
For high-risk individuals (hereditary chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis), consider EUS.
Frequency not specified
UK:[9]
For hereditary chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, consider annual monitoring for pancreatic cancer
OsteopeniaOsteopeniaOsteoporosis and osteoporosisOsteoporosisOsteoporosis refers to a decrease in bone mass and density leading to an increased number of fractures. There are 2 forms of osteoporosis: primary, which is commonly postmenopausal or senile; and secondary, which is a manifestation of immobilization, underlying medical disorders, or long-term use of certain medications. Osteoporosis
Fat-soluble vitaminFat-soluble VitaminFat-soluble vitamins are absorbed and stored in adipose tissue (fat) and the liver. These vitamins can be released from storage and used when necessary. The 4 important fat-soluble vitamins are A, D, E, and K. Fat-soluble Vitamins and their Deficiencies deficiencies (A, D, E, K)
Pancreatic diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus
Structural:[7,10–12]
Pancreatic pseudocystPancreatic pseudocystCyst-like space not lined by epithelium and contained within the pancreas. Pancreatic pseudocysts account for most of the cystic collections in the pancreas and are often associated with chronic pancreatitis.Acute Cholangitisformation (encapsulatedEncapsulatedKlebsiella collection of fluid)
Usually self-resolves, but may be complicated by infection or rupture
Can be drained if > 5 cm or symptomatic
BileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct and duodenal obstruction from direct compressionCompressionBlunt Chest Trauma from a pseudocyst
PseudoaneurysmPseudoaneurysmNot an aneurysm but a well-defined collection of blood and connective tissue outside the wall of a blood vessel or the heart. It is the containment of a ruptured blood vessel or heart, such as sealing a rupture of the left ventricle. False aneurysm is formed by organized thrombus and hematoma in surrounding tissue.Thoracic Aortic Aneurysms develops when there is erosionErosionPartial-thickness loss of the epidermisGeneralized and Localized Rashes of an artery into a pseudocyst (potentially life-threatening!)
Splenic or portal veinPortal veinA short thick vein formed by union of the superior mesenteric vein and the splenic vein.Liver: AnatomythrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus due to inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation surrounding the veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology
Pancreatic ductal adenocarcinomaPancreatic Ductal AdenocarcinomaChronic Pancreatitis from chronic inflammationChronic InflammationInflammation (higher risk in hereditary forms of pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis)
Pancreatic pseudocyst: CT scan of the abdomen, after oral and IV contrast, showing a cystic lesion in the region of the tail of pancreas, suggestive of pancreatic pseudocyst
Image: “CT scan abdomen” by Department of Medical Gastroenterology, Medical College, Trivandrum, Kerala, India. License: CC BY 2.0
CholelithiasisCholelithiasisCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant). Cholelithiasis: presence of gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis within the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy. May be asymptomatic or present with colicky right upper quadrantRight upper quadrantAnterior Abdominal Wall: Anatomyabdominal painAbdominal PainAcute Abdomen, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. Biliary tractBiliary tractBile is secreted by hepatocytes into thin channels called canaliculi. These canaliculi lead into slightly larger interlobular bile ductules, which are part of the portal triads at the “corners” of hepatic lobules. The bile leaves the liver via the right and left hepatic ducts, which join together to form the common hepatic duct. Gallbladder and Biliary Tract: Anatomy stones are visualized by ultrasound or CT. Treatment involves diet modification, painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control, and cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy for symptomatic individuals. Symptoms and imaging will differentiate this condition from chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
PerforationPerforationA pathological hole in an organ, blood vessel or other soft part of the body, occurring in the absence of external force.Esophagitis of the intestine: injury of the bowel wall, resulting in subsequent release of gastrointestinal contents into the peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may present with acute chest or abdominal painAbdominal PainAcute Abdomen and display evidence of peritonitisPeritonitisInflammation of the peritoneum lining the abdominal cavity as the result of infectious, autoimmune, or chemical processes. Primary peritonitis is due to infection of the peritoneal cavity via hematogenous or lymphatic spread and without intra-abdominal source. Secondary peritonitis arises from the abdominal cavity itself through rupture or abscess of intra-abdominal organs.Penetrating Abdominal Injury. Computed tomography will show extraluminal gas. Management usually involves antibiotics and surgery. Physical exam and imaging will differentiate this condition from chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Chronic mesenteric ischemiaChronic Mesenteric IschemiaMesenteric Ischemia: caused by inadequate blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure through the mesenteric vessels, resulting in ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage of the bowel wall. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with episodic, postprandial abdominal painAbdominal PainAcute Abdomen, and may lose weight due to food aversionFood aversionIntestinal Ischemia. Computed tomography angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery is used for diagnosis, and treatment may include conservative measures or revascularizationRevascularizationThromboangiitis Obliterans (Buerger Disease). Imaging will differentiate this condition from chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Peptic ulcerPeptic ulcerPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease disease: a gastric (or duodenal) mucosal defect resulting from gastric acidGastric acidHydrochloric acid present in gastric juice.Gastroesophageal Reflux Disease (GERD) hypersecretion or impaired bicarbonateBicarbonateInorganic salts that contain the -HCO3 radical. They are an important factor in determining the ph of the blood and the concentration of bicarbonate ions is regulated by the kidney. Levels in the blood are an index of the alkali reserve or buffering capacity.ElectrolytessecretionSecretionCoagulation Studies. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may have dyspepsiaDyspepsiaImpaired digestion, especially after eating.Lactose Intolerance, postprandial painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, early satietyEarly SatietyBariatric Surgery, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, or evidence of bleeding. Diagnosis is made with upper endoscopyEndoscopyProcedures of applying endoscopes for disease diagnosis and treatment. Endoscopy involves passing an optical instrument through a small incision in the skin i.e., percutaneous; or through a natural orifice and along natural body pathways such as the digestive tract; and/or through an incision in the wall of a tubular structure or organ, i.e. Transluminal, to examine or perform surgery on the interior parts of the body.Gastroesophageal Reflux Disease (GERD). Management includes lifestyle changes, Helicobacter pyloriHelicobacter pyloriA spiral bacterium active as a human gastric pathogen. It is a gram-negative, urease-positive, curved or slightly spiral organism initially isolated in 1982 from patients with lesions of gastritis or peptic ulcers in Western Australia. Helicobacter pylori was originally classified in the genus campylobacter, but RNA sequencing, cellular fatty acid profiles, growth patterns, and other taxonomic characteristics indicate that the micro-organism should be included in the genus Helicobacter. It has been officially transferred to Helicobacter gen.Helicobacter treatment, and proton pumpPumpACES and RUSH: Resuscitation Ultrasound Protocols inhibitors. The history and endoscopic findings will differentiate this condition from chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Pancreatic cancer: a malignancyMalignancyHemothorax of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy tissue. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may be asymptomatic at first, but can later develop vague, chronic epigastric painEpigastric painMallory-Weiss Syndrome (Mallory-Weiss Tear); weight lossWeight lossDecrease in existing body weight.Bariatric Surgery; steatorrheaSteatorrheaA condition that is characterized by chronic fatty diarrhea, a result of abnormal digestion and/or intestinal absorption of fats.Diarrhea; and jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice. Diagnosis is made with abdominal imaging, biopsyBiopsyRemoval and pathologic examination of specimens from the living body.Ewing Sarcoma, and tumorTumorInflammation markers. Treatment depends on the cancer type and stagingStagingMethods which attempt to express in replicable terms the extent of the neoplasm in the patient.Grading, Staging, and Metastasis. Chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute PancreatitispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship (particularly those with hereditary forms) are at risk for pancreatic cancer.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, a long-standing inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy that leads to irreversible damage and loss of functionLoss of FunctionInflammation. Codes can specify the cause, such as alcohol-induced.
Coding System
Code
Description
ICD-10-CM
K86.1
Other chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
ICD-10-CM
K86.0
Alcohol-induced chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Evaluation & Workup:
These codes are for imaging studies used to diagnose the structural changes of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, such as calcifications, ductal dilation, and atrophyAtrophyDecrease in the size of a cell, tissue, organ, or multiple organs, associated with a variety of pathological conditions such as abnormal cellular changes, ischemia, malnutrition, or hormonal changes.Cellular Adaptation. A CT scan is often used, while an MRCPMRCPNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis provides detailed images of the pancreatic ducts.
Coding System
Code
Description
CPT
74177
Computed tomography, abdomen and pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy; with contrast material(s)
CPT
74181
Magnetic resonance (eg, proton) imaging, abdomen; without contrast material(s)
Medications:
This code is for pancreatic enzyme replacementEnzyme replacementTherapeutic replacement or supplementation of defective or missing enzymes to alleviate the effects of enzyme deficiency (e.g., glucosylceramidase replacement for gaucher disease).Severe Combined Immunodeficiency (SCID) therapy (PERT), a cornerstone of treatment for the exocrine insufficiency caused by chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis. These enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes help patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship digest food properly.
Coding System
Code
Description
RxNorm
243575
Pancrelipase
Complications:
These codes document the major long-term consequences of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis: exocrine pancreatic insufficiencyExocrine pancreatic insufficiencyA malabsorption condition resulting from greater than 10% reduction in the secretion of pancreatic digestive enzymes (lipase; proteases; and amylase) by the exocrine pancreas into the duodenum. This condition is often associated with cystic fibrosis and with chronic pancreatitis.Malabsorption and Maldigestion leading to malabsorptionMalabsorptionGeneral term for a group of malnutrition syndromes caused by failure of normal intestinal absorption of nutrients.Malabsorption and Maldigestion, and destruction of islet cells leading to diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus.
Coding System
Code
Description
ICD-10-CM
K86.81
Exocrine pancreatic insufficiencyExocrine pancreatic insufficiencyA malabsorption condition resulting from greater than 10% reduction in the secretion of pancreatic digestive enzymes (lipase; proteases; and amylase) by the exocrine pancreas into the duodenum. This condition is often associated with cystic fibrosis and with chronic pancreatitis.Malabsorption and Maldigestion
ICD-10-CM
E13.9
Other specified diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus without complications
Brock, C., Nielsen, L. M., Lelic, D., Drewes, A. M. (2013). Pathophysiology of chronic pancreatitis. World Journal of Gastroenterology, 19(42), 7231–7240. https://doi.org/10.3748/wjg.v19.i42.7231
Kasper, D. L., Fauci, A. S., Longo, D. L., Bruanwald, E., Hauser, S. L., Jameson, J. L. (2007). Harrison’s Principles of Internal Medicine (16th edition.). New York: McGraw-Hill Education.
Conwell, D. L., Lee, L. S., Yadav, D., et al. (2014). American Pancreatic Association practice guidelines in chronic pancreatitis: evidence-based report on diagnostic guidelines. Pancreas, 43(8), 1143–1162. https://doi.org/10.1097/MPA.0000000000000237
Singh, V. K., Yadav, D., Garg, P. K. (2019). Diagnosis and management of chronic pancreatitis: a review. JAMA, 322(24), 2422. https://doi.org/10.1001/jama.2019.19411
Lohr, J. M., et al. (2017). United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis. United European Gastroenterology Journal, 5(2), 153–199. https://journals.sagepub.com/doi/pdf/10.1177/2050640616684695
Shimizu, K., et al. (2022). Evidence-based clinical practice guidelines for chronic pancreatitis 2021. Journal of Gastroenterology, 57(10):709–24. https://doi.org/10.1007/s00535-022-01911-6
Conwell DL, et al. (2018). Acute and Chronic Pancreatitis, in Harrison’s Principles of Internal Medicine. 20th ed., pp 2444-45. Eds: Jameson, J. L., Fauci, A. S., Kasper, D. L., et al.
Robbins and Cotran Pathologic Basis of Disease (2021). E-book, Kindle edition, locations 39919-90. https://read.amazon.com/?ref_=dbs_p_ebk_r00_pbcb_rnvc00&_encoding=UTF8&asin=B0892Q533V
Whitcomb, D. C. (2022). Central role of the sentinel acute pancreatitis event (SAPE) model in understanding recurrent acute pancreatitis (RAP): Implications for precision medicine. Frontiers in Pediatrics, 10. https://www.frontiersin.org/articles/10.3389/fped.2022.941852
Create your free account or log in to continue reading!