Cellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. The borders are not clearly delineated. The lower extremities are the most frequent site of infection, but cellulitis can occur anywhere on the body. Diagnosis is usually clinical, and management involves oral and/or parenteral antibiotics. Coverage for MRSA may be added, depending on the presence of risk factors.
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis is inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and subcutaneous tissues. It is often due to infection.
Epidemiology and etiology[1‒3]
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency: 200 cases per 100,000 patient-years
More common in middle-aged and older populations
Lower extremities: most common site
Most common agents:
Staphylococcus aureusStaphylococcus aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Brain Abscess:
MSSA
MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus
Group A StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus (StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus pyogenes)
Less common agents:
Pasteurellamultocida (from animal bites)
Aeromonas hydrophilaAeromonas hydrophilaA species of gram-negative, facultatively anaerobic, rod-shaped bacteria that may be pathogenic for frogs, fish, and mammals, including man. In humans, cellulitis and diarrhea can result from infection with this organism.Cellulitis and Vibrio vulnificusVibrio vulnificusA species of halophilic bacteria in the genus vibrio, which lives in warm seawater. It can cause infections in those who eat raw contaminated seafood or have open wounds exposed to seawater.Vibrio (after water exposure)
Clostridium species (myonecrosisMyonecrosisA severe condition resulting from bacteria invading healthy muscle from adjacent traumatized muscle or soft tissue. The infection originates in a wound contaminated with bacteria of the genus Clostridium. C. perfringens accounts for the majority of cases (over eighty percent), while C. novyi, C. septicum, and C. histolyticum cause most of the other cases.Clostridia)
Pseudomonas aeruginosaPseudomonas aeruginosaA species of gram-negative, aerobic, rod-shaped bacteria commonly isolated from clinical specimens (wound, burn, and urinary tract infections). It is also found widely distributed in soil and water. P. Aeruginosa is a major agent of nosocomial infection.Pseudomonas (in immunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.GastroenteritispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
ErysipelothrixErysipelothrixA genus of gram-positive, facultatively anaerobic, rod-shaped bacteria that has a tendency to form long filaments. Its organisms are widely distributed in nature and are found in mammals; birds; and fishes. Erysipelothrix may appear gram-negative because they decolorize easily.Cellulitis rhusiopathiae (occupational exposure in butchers, slaughterhouse workers, farmers, veterinarians)
Risk factors[2]
Breach of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions barrier (wounds, ulcers, insect/animal bites)
SkinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and FunctionsinflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation (psoriasisPsoriasisPsoriasis is a common T-cell-mediated inflammatory skin condition. The etiology is unknown, but is thought to be due to genetic inheritance and environmental triggers. There are 4 major subtypes, with the most common form being chronic plaque psoriasis. Psoriasis, eczemaEczemaAtopic dermatitis, also known as eczema, is a chronic, relapsing, pruritic, inflammatory skin disease that occurs more frequently in children, although adults can also be affected. The condition is often associated with elevated serum levels of IgE and a personal or family history of atopy. Skin dryness, erythema, oozing, crusting, and lichenification are present. Atopic Dermatitis (Eczema))
Injuries contaminated with dirt or seawater
Preexisting infection (tinea, varicella)
Previous history of cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis
Crush injuries
Second- and third-degree burnsBurnsA burn is a type of injury to the skin and deeper tissues caused by exposure to heat, electricity, chemicals, friction, or radiation. Burns are classified according to their depth as superficial (1st-degree), partial-thickness (2nd-degree), full-thickness (3rd-degree), and 4th-degree burns. Burns
FrostbiteFrostbiteInjuries due to cold weather are common among children and athletes who are involved in sports played in cold conditions. Frostbite is a direct freezing injury to the peripheral tissues and occurs when the skin temperature drops below 0°C (32°F). Common sites of frostbite include the nose, ears, fingers, and toes. Frostbite
DiabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus mellitus
ObesityObesityObesity is a condition associated with excess body weight, specifically with the deposition of excessive adipose tissue. Obesity is considered a global epidemic. Major influences come from the western diet and sedentary lifestyles, but the exact mechanisms likely include a mixture of genetic and environmental factors. Obesity
BacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology enter disrupted skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions barrier:
Through minor cuts or injuries
May be secondary to a distant site or systemic infection
In some cases, portal of entry is not evident.
Invasion of dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions and subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess triggers cytokine release, recruiting neutrophilsNeutrophilsGranular leukocytes having a nucleus with three to five lobes connected by slender threads of chromatin, and cytoplasm containing fine inconspicuous granules and stainable by neutral dyes.Innate Immunity: Phagocytes and Antigen Presentation and other inflammatory cells to the site.
Intrinsic bacterial factors allow the pathogen to evade initial host defenses, leading to erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion, painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and local swellingSwellingInflammation of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions (edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema).
Infection is generally limited to the area of invasion.
If the pathogen overcomes the immune defenses, further spread (deeper and/or contiguous infection and bacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides in immunodeficiencyImmunodeficiencyChédiak-Higashi Syndrome) occurs.
Reduced control of infection occurs in:
Decreased tissue vascularity and oxygenation
Increased peripheral fluid stasis
Poor ability to combat infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., diabetesDiabetesDiabetes mellitus (DM) is a metabolic disease characterized by hyperglycemia and dysfunction of the regulation of glucose metabolism by insulin. Type 1 DM is diagnosed mostly in children and young adults as the result of autoimmune destruction of β cells in the pancreas and the resulting lack of insulin. Type 2 DM has a significant association with obesity and is characterized by insulin resistance.Diabetes Mellitus)
Clinical findings[1,2]
Prodromal systemic symptoms:
May have signs of toxicityToxicityDosage Calculation (feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever > 100.5℉ (38℃), chillsChillsThe sudden sensation of being cold. It may be accompanied by shivering.Fever, and tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children)
Muscle and joint painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways
HeadacheHeadacheThe symptom of pain in the cranial region. It may be an isolated benign occurrence or manifestation of a wide variety of headache disorders.Brain Abscess
Local features:
Indurated lesions or edematous area with erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion and poorly defined borders
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways and tenderness in the affected area
Tight, glossy, swollen skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions or dimpling (noted in edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema surrounding hair follicles)
May present with purulent exudateExudateExudates are fluids, cells, or other cellular substances that are slowly discharged from blood vessels usually from inflamed tissues.Pleural Effusion (usually associated with S. aureusS. aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Staphylococcus)
An abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease may also be found (collection of pus within the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions or subcutaneous layer).
Severe infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease:
Can present with general malaiseMalaiseTick-borne Encephalitis Virus, fatigueFatigueThe state of weariness following a period of exertion, mental or physical, characterized by a decreased capacity for work and reduced efficiency to respond to stimuli.Fibromyalgia, dizzinessDizzinessAn imprecise term which may refer to a sense of spatial disorientation, motion of the environment, or lightheadedness.Lateral Medullary Syndrome (Wallenberg Syndrome), confusion, muscle and joint painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and diaphoresis
Abdominal wall cellulitis: Image shows marked pitting edema and erythema with poorly demarcated borders due to cellulitis.
Image: “How 40 kilograms of fluid retention can be overlooked: two case reports” by Ong HS, Sze CW, Koh TW, Coppack SW. License: CC BY 2.0
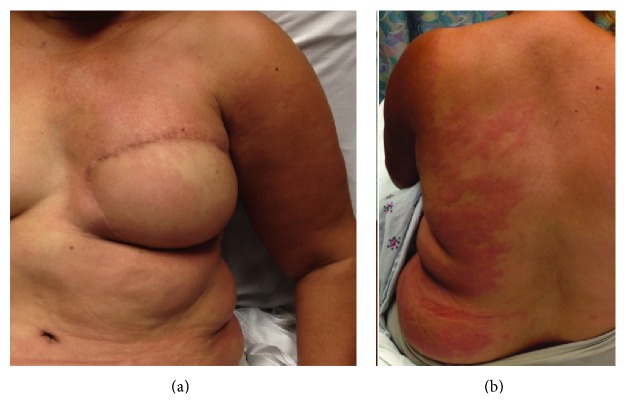
Lymphedema cellulitis: Stagnant lymph is an ideal medium for bacterial growth, and progression can be rapid owing to a decreased ability to fight infection in the affected area. Infections are commonly caused by gram-positive cocci bacteria.
Image: “A Woman with Unilateral Rash and Fever: Cellulitis in the Setting of Lymphedema” by Joseph M, Camilon M, Kang T. License: CC BY 3.0
Diagnosis
Diagnosis of cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis is clinical:[6–8]
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
ErythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion
Warmth
Tenderness
Associated lymphadenopathyLymphadenopathyLymphadenopathy is lymph node enlargement (> 1 cm) and is benign and self-limited in most patients. Etiologies include malignancy, infection, and autoimmune disorders, as well as iatrogenic causes such as the use of certain medications. Generalized lymphadenopathy often indicates underlying systemic disease. Lymphadenopathy
Symptoms, risk factors, and progression of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions lesion aid in ruling out differential diagnoses.
Laboratory tests are nonspecific:[6–8]
LeukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus (common in all infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease)
Obtaining skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions cultures is not recommended unless the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions is broken.[6]
Wound culture: used to identify pathogens and guide antibiotic therapy
Blood culture: obtained in cases suggestive of bacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides or sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock and in severely immunodeficient patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship[6]
Imaging:[6–8]
Ultrasonography (US) is used to rule out abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease.
Complicated skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and soft tissueSoft TissueSoft Tissue AbscessinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease need to be further evaluated.
Orbital and sinus CT to determine extent of orbital cellulitisOrbital cellulitisOrbital and preseptal cellulitis are infections differentiated by the anatomic sites affected in the orbit. Infection posterior to the septum is orbital cellulitis. Inoculation with the pathogen can occur through trauma or surgery. Cellulitis also occurs via extension from a nearby structure (such as from sinus infection or sinusitis). Orbital and Preseptal Cellulitis and presence of an abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease
MRI and/or boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and TypesscintigraphyScintigraphySjögren Syndrome may be performed in cases of severe joint painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways to confirm/rule out septic arthritisArthritisAcute or chronic inflammation of joints.Osteoarthritis or osteomyelitisOsteomyelitisOsteomyelitis is an infection of the bone that results from the spread of microorganisms from the blood (hematogenous), nearby infected tissue, or open wounds (non-hematogenous). Infections are most commonly caused by Staphylococcus aureus.Osteomyelitis.
Antibiotic protocols may vary based on the microbiologic susceptibility of the population of the practice location. The following recommendations are based on US and UK guidelines.
Treatment approach
Use a marking pen to draw around the borders of the initial infected site to track progression of disease.[5‒7]
Supportive care:[5‒9]
Symptomatic treatment for feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, local painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and aches
Adequate hydration and elevation of the affected extremity
Empiric therapyEmpiric TherapyMeningitis in Children covers group A StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus and MSSA.[5‒7]
Determination of risk factors and need for parenteral therapy:[5‒7]
MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus risk factors:
Recent hospitalizationHospitalizationThe confinement of a patient in a hospital.Delirium or surgery (≤ 2 months ago)
HemodialysisHemodialysisProcedures which temporarily or permanently remedy insufficient cleansing of body fluids by the kidneys.Crush Syndrome
Prior episode of MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus
Recent antibiotic use without MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus coverage
Rapid progression of erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis over a medical device (vascular graftVascular graftSurgical insertion of blood vessel prostheses, or transplanted blood vessels, or other biological material to repair injured or diseased blood vessels.Peritoneal Dialysis and Hemodialysis or prosthetic joint)
Failure to respond to prior oral antibiotics
Treatment regimen
General principles:[6–8]
Recommended duration of antibiotic intake is generally 5–7 days, but this can be prolonged if resolution is not achieved in that time period.
When improvement is noted, switch parenteral regimen to oral antibiotics.
No MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus risk factors (Table 1):
Oral therapy (mild infection):
Flucloxacillin (not available in the US)[7]
DicloxacillinDicloxacillinOne of the penicillins which is resistant to penicillinase.Penicillins[2,6–8]
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins–clavulanate[1,4,6]
UK: erythromycinErythromycinA bacteriostatic antibiotic macrolide produced by streptomyces erythreus. Erythromycin a is considered its major active component. In sensitive organisms, it inhibits protein synthesis by binding to 50s ribosomal subunits. This binding process inhibits peptidyl transferase activity and interferes with translocation of amino acids during translation and assembly of proteins.Macrolides and Ketolides (alternative for penicillinPenicillinRheumatic FeverallergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction; use in pregnancyPregnancyThe status during which female mammals carry their developing young (embryos or fetuses) in utero before birth, beginning from fertilization to birth.Pregnancy: Diagnosis, Physiology, and Care)[7]
UK: clarithromycinClarithromycinA semisynthetic macrolide antibiotic derived from erythromycin that is active against a variety of microorganisms. It can inhibit protein synthesis in bacteria by reversibly binding to the 50s ribosomal subunits. This inhibits the translocation of aminoacyl transfer-RNA and prevents peptide chain elongation.Macrolides and Ketolides (alternative for penicillinPenicillinRheumatic FeverallergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction)[7]
CefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporins[6]
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides[6–8]
With MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus risk factors (Table 2):
Oral therapy:
TrimethoprimTrimethoprimThe sulfonamides are a class of antimicrobial drugs inhibiting folic acid synthesize in pathogens. The prototypical drug in the class is sulfamethoxazole. Although not technically sulfonamides, trimethoprim, dapsone, and pyrimethamine are also important antimicrobial agents inhibiting folic acid synthesis. The agents are often combined with sulfonamides, resulting in a synergistic effect. Sulfonamides and Trimethoprim–sulfamethoxazoleSulfamethoxazoleA bacteriostatic antibacterial agent that interferes with folic acid synthesis in susceptible bacteria. Its broad spectrum of activity has been limited by the development of resistance.Sulfonamides and Trimethoprim[6]
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins plus doxycycline[7,8]
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides[6–8]
LinezolidLinezolidAn oxazolidinone and acetamide derived anti-bacterial agent and protein synthesis inhibitor that is used in the treatment of gram-positive bacterial infections of the skin and respiratory tract.Oxazolidinones[6–8]
Parenteral therapy:
VancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides (1st choice)[6–8]
TeicoplaninTeicoplaninLipoglycopeptide antibiotic from actinoplanes teichomyceticus active against gram-positive bacteria. It consists of five major components each with a different fatty acid moiety.Glycopeptides (UK)[7,8]
LinezolidLinezolidAn oxazolidinone and acetamide derived anti-bacterial agent and protein synthesis inhibitor that is used in the treatment of gram-positive bacterial infections of the skin and respiratory tract.Oxazolidinones[6–8]
Other considerations:
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis around the eye:[8]
Differentiate preseptal (periorbitalPeriorbitalOrbital and Preseptal Cellulitis) from orbital cellulitisOrbital cellulitisOrbital and preseptal cellulitis are infections differentiated by the anatomic sites affected in the orbit. Infection posterior to the septum is orbital cellulitis. Inoculation with the pathogen can occur through trauma or surgery. Cellulitis also occurs via extension from a nearby structure (such as from sinus infection or sinusitis). Orbital and Preseptal Cellulitis.
Orbital cellulitisOrbital cellulitisOrbital and preseptal cellulitis are infections differentiated by the anatomic sites affected in the orbit. Infection posterior to the septum is orbital cellulitis. Inoculation with the pathogen can occur through trauma or surgery. Cellulitis also occurs via extension from a nearby structure (such as from sinus infection or sinusitis). Orbital and Preseptal Cellulitis, which involves deeper tissues, can lead to visionVisionOphthalmic Exam loss and/or life-threatening complications.
Co-management with ophthalmology is recommended.
Bite wounds: add anaerobic coverage
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins–clavulanate (1st-line therapy; covers both aerobic and anaerobic organisms)
Can add metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess or clindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides to alternative agents (if penicillinPenicillinRheumatic FeverallergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction present)
Usually required for facial lesions because of high risk of spread of infection to the CNS (meningitisMeningitisMeningitis is inflammation of the meninges, the protective membranes of the brain, and spinal cord. The causes of meningitis are varied, with the most common being bacterial or viral infection. The classic presentation of meningitis is a triad of fever, altered mental status, and nuchal rigidity. Meningitis, encephalitisEncephalitisEncephalitis is inflammation of the brain parenchyma caused by an infection, usually viral. Encephalitis may present with mild symptoms such as headache, fever, fatigue, and muscle and joint pain or with severe symptoms such as seizures, altered consciousness, and paralysis.Encephalitis)
For those with concomitant conditions such as hepatic, renal, or cardiac failureCardiac failureCongestive heart failure refers to the inability of the heart to supply the body with normal cardiac output to meet metabolic needs. Echocardiography can confirm the diagnosis and give information about the ejection fraction.Heart Failure
Severe progressive infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (might require surgical debridementDebridementThe removal of foreign material and devitalized or contaminated tissue from or adjacent to a traumatic or infected lesion until surrounding healthy tissue is exposed.Stevens-Johnson Syndrome of necrotic tissue or abscesses):
An example is infection involving the perineumPerineumThe body region lying between the genital area and the anus on the surface of the trunk, and to the shallow compartment lying deep to this area that is inferior to the pelvic diaphragm. The surface area is between the vulva and the anus in the female, and between the scrotum and the anus in the male.Vagina, Vulva, and Pelvic Floor: Anatomy and genitalia.[6]
Necrotizing infection (Fournier gangreneFournier gangreneAn acute necrotic infection of the scrotum; penis; or perineum. It is characterized by scrotum pain and redness with rapid progression to gangrene and sloughing of tissue. Fournier gangrene is usually secondary to perirectal or periurethral infections associated with local trauma, operative procedures, or urinary tract disease.Necrotizing Fasciitis) involving the perineumPerineumThe body region lying between the genital area and the anus on the surface of the trunk, and to the shallow compartment lying deep to this area that is inferior to the pelvic diaphragm. The surface area is between the vulva and the anus in the female, and between the scrotum and the anus in the male.Vagina, Vulva, and Pelvic Floor: Anatomy/penisPenisThe penis is the male organ of copulation and micturition. The organ is composed of a root, body, and glans. The root is attached to the pubic bone by the crura penis. The body consists of the 2 parallel corpora cavernosa and the corpus spongiosum. The glans is ensheathed by the prepuce or foreskin. Penis: Anatomy/labia carries a high mortalityMortalityAll deaths reported in a given population.Measures of Health Status rate.
Suspicion should prompt emergent surgical consult.
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis with severe sepsisSevere SepsisSepsis in Children or immunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.Gastroenteritis state (e.g., neutropeniaNeutropeniaNeutrophils are an important component of the immune system and play a significant role in the eradication of infections. Low numbers of circulating neutrophils, referred to as neutropenia, predispose the body to recurrent infections or sepsis, though patients can also be asymptomatic. Neutropenia) is initially treated with vancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides PLUS:[6–8]
MeropenemMeropenemA thienamycin derivative antibacterial agent that is more stable to renal dehydropeptidase I than imipenem, but does not need to be given with an enzyme inhibitor such as cilastatin. It is used in the treatment of bacterial infections, including infections in immunocompromised patients.Carbapenems and Aztreonam 1 g IV every 8 hours (for suspected ESBLESBLKlebsiella infection) OR
PiperacillinPiperacillinSemisynthetic, broad-spectrum, ampicillin derived ureidopenicillin antibiotic proposed for pseudomonas infections. It is also used in combination with other antibiotics.Penicillins–tazobactamTazobactamA penicillanic acid and sulfone derivative and potent beta-lactamase inhibitor that enhances the activity of other anti-bacterial agents against beta-lactamase producing bacteria.Cephalosporins 4.5 g IV every 6–8 hours
Recurrent cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis (3–4 episodes/year):[6–8]
PenicillinPenicillinRheumatic Fever VK: 250–500 mg by mouth, 2 times/day, after treatment of the acute infection, for 4–52 weeks
ErythromycinErythromycinA bacteriostatic antibiotic macrolide produced by streptomyces erythreus. Erythromycin a is considered its major active component. In sensitive organisms, it inhibits protein synthesis by binding to 50s ribosomal subunits. This binding process inhibits peptidyl transferase activity and interferes with translocation of amino acids during translation and assembly of proteins.Macrolides and Ketolides: 250 mg by mouth, 2 times/day, after treatment of the acute infection, for 4–52 weeks
Table 1: Treatment regimen for cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis (no MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus risk factors)
DicloxacillinDicloxacillinOne of the penicillins which is resistant to penicillinase.Penicillins[2,6–8]
25–50 mg/kg/day in 4 divided doses; maximum, 500 mg/dose
250 mg‒500 mg 4 times/day; maximum, 2 g/day
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins–clavulanate[1–4,6]
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides[6-8]
25–30 mg/kg/day in 3 divided doses
300‒450 mg 4 times/day
ClarithromycinClarithromycinA semisynthetic macrolide antibiotic derived from erythromycin that is active against a variety of microorganisms. It can inhibit protein synthesis in bacteria by reversibly binding to the 50s ribosomal subunits. This inhibits the translocation of aminoacyl transfer-RNA and prevents peptide chain elongation.Macrolides and Ketolidesa[7]
1 month–11 years old: 7.5 mg/kg every 12 hours, maximum, 500 mg/dose
> 11 years: 250–500 mg 2 times/day
500 mg 2 times/day
ErythromycinErythromycinA bacteriostatic antibiotic macrolide produced by streptomyces erythreus. Erythromycin a is considered its major active component. In sensitive organisms, it inhibits protein synthesis by binding to 50s ribosomal subunits. This binding process inhibits peptidyl transferase activity and interferes with translocation of amino acids during translation and assembly of proteins.Macrolides and Ketolidesa[7]
> 8 years old: 250–500 mg 4 times/day
500 mg 4 times/day
Doxycyclinea[6–8]
≥ 8 years old: 2 mg/kg every 12 hours; maximum, 100 mg/dose
CefazolinCefazolinA semisynthetic cephalosporin analog with broad-spectrum antibiotic action due to inhibition of bacterial cell wall synthesis. It attains high serum levels and is excreted quickly via the urine.Cephalosporinsb[6]
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides[6–8]
25–40 mg/kg/day in 3 divided doses
600 mg every 8 hours
aUK recommendations
bMay be given in cases of penicillin allergy, except in those with immediate hypersensitivity reactions
Table 2: Treatment regimen for cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis (with MRSAMRSAA strain of Staphylococcus aureus that is non-susceptible to the action of methicillin. The mechanism of resistance usually involves modification of normal or the presence of acquired penicillin binding proteins.Staphylococcus risk factors)
Medication
Pediatric dose
Adult dose
Oral therapy
TrimethoprimTrimethoprimThe sulfonamides are a class of antimicrobial drugs inhibiting folic acid synthesize in pathogens. The prototypical drug in the class is sulfamethoxazole. Although not technically sulfonamides, trimethoprim, dapsone, and pyrimethamine are also important antimicrobial agents inhibiting folic acid synthesis. The agents are often combined with sulfonamides, resulting in a synergistic effect. Sulfonamides and Trimethoprim–sulfamethoxazoleSulfamethoxazoleA bacteriostatic antibacterial agent that interferes with folic acid synthesis in susceptible bacteria. Its broad spectrum of activity has been limited by the development of resistance.Sulfonamides and Trimethoprim[6]
8–12 mg/kg/day in 2 divided doses (based on trimethoprimTrimethoprimThe sulfonamides are a class of antimicrobial drugs inhibiting folic acid synthesize in pathogens. The prototypical drug in the class is sulfamethoxazole. Although not technically sulfonamides, trimethoprim, dapsone, and pyrimethamine are also important antimicrobial agents inhibiting folic acid synthesis. The agents are often combined with sulfonamides, resulting in a synergistic effect. Sulfonamides and Trimethoprim component)
1–2 double-strength tablets 2 times daily
AmoxicillinAmoxicillinA broad-spectrum semisynthetic antibiotic similar to ampicillin except that its resistance to gastric acid permits higher serum levels with oral administration.Penicillins plus doxycycline[[7,8]
See individual dosing in Table 1.
See individual dosing in Table 1.
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides[6-8]
See individual dosing in Table 1.
See individual dosing in Table 1.
Parenteral therapy
VancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides[6–8]
10–15 mg/kg 4 times a day, adjusted to vancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides concentration
15–20 mg/kg 2–3 times a day, adjusted to vancomycinVancomycinAntibacterial obtained from streptomyces orientalis. It is a glycopeptide related to ristocetin that inhibits bacterial cell wall assembly and is toxic to kidneys and the inner ear.Glycopeptides concentration
TeicoplaninTeicoplaninLipoglycopeptide antibiotic from actinoplanes teichomyceticus active against gram-positive bacteria. It consists of five major components each with a different fatty acid moiety.Glycopeptidesa[7,8]
1 month: 16 mg/kg for once, then after 24 hours, 8 mg/kg once a day
2 months–11 years old: 10 mg/kg every 12 hours for 3 doses, then 6–10 mg/kg once a day
12–17 years: 6 mg/kg every 12 hours for 3 doses, then 6 mg/kg daily
6 mg/kg every 12 hours for 3 doses, then every 24 hours
LinezolidLinezolidAn oxazolidinone and acetamide derived anti-bacterial agent and protein synthesis inhibitor that is used in the treatment of gram-positive bacterial infections of the skin and respiratory tract.Oxazolidinones[6-8]
10 mg/kg every 12 hours
600 mg 2 times/day
aUK recommendations
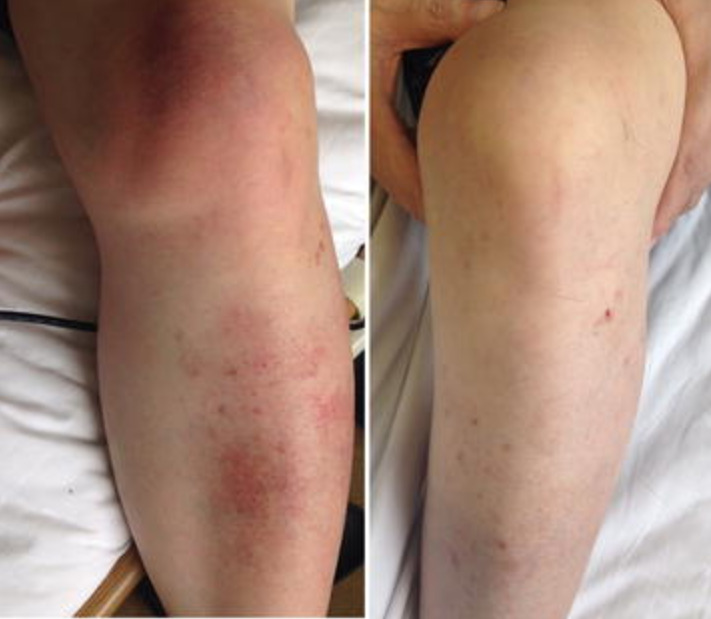
Cellulitis in the left lower leg and knee: Left: Local swelling with salmon-pink skin discoloration and local warmth is evident. Right: leg after 6 weeks of antibiotic therapy
Image: “Helicobacter cinaedi bacteremia with cellulitis in a living-donor kidney transplant recipient identified by matrix-assisted laser desorption ionization time-of-flight mass spectrometry: a case report” by BMC Research Notes. License: CC BY 4.0
Complications[5,8]
AbscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease:
Collection of pus in the dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions or subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess
Treatment: incision and drainageIncision And DrainageChalazion of drainable abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease detected on exam or US
Necrotizing fasciitisNecrotizing fasciitisNecrotizing fasciitis is a life-threatening infection that causes rapid destruction and necrosis of the fascia and subcutaneous tissues. Patients may present with significant pain out of proportion to the presenting symptoms and rapidly progressive erythema of the affected area. Necrotizing Fasciitis:
Deep infection associated with rapid destruction and necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage of the fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis and subcutaneous tissues
Infection in a joint, frequently secondary to bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology
Develops from hematogenous seedingHematogenous SeedingSeptic Arthritis but can also arise from extensionExtensionExamination of the Upper Limbs of infection from the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions/soft tissueSoft TissueSoft Tissue Abscess
OsteomyelitisOsteomyelitisOsteomyelitis is an infection of the bone that results from the spread of microorganisms from the blood (hematogenous), nearby infected tissue, or open wounds (non-hematogenous). Infections are most commonly caused by Staphylococcus aureus.Osteomyelitis:
Infection of the boneBoneBone is a compact type of hardened connective tissue composed of bone cells, membranes, an extracellular mineralized matrix, and central bone marrow. The 2 primary types of bone are compact and spongy. Bones: Structure and Types
Poorly healing skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and soft tissueSoft TissueSoft Tissue AbscessinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease are at risk.
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock:
Potentially life-threatening organ dysfunction caused by a dysregulated host response to infection
Presentation can include feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children, tachypneaTachypneaIncreased respiratory rate.Pulmonary Examination, hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension, and/or altered mentation.
ImmunocompromisedimmunocompromisedA human or animal whose immunologic mechanism is deficient because of an immunodeficiency disorder or other disease or as the result of the administration of immunosuppressive drugs or radiation.GastroenteritispatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and FunctionsinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease are at risk for this condition.
ErysipelasErysipelasErysipelas is a bacterial infection of the superficial layer of the skin extending to the skin’s superficial lymphatic vessels. This infection presents as a raised, well-defined, tender, and bright red rash. Typically on the legs or face, but erysipelas can occur anywhere on the skin. Erysipelas: an acute superficial infection of the upper dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions and lymphatics, usually caused by group A beta-hemolyticStreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus: This condition presents as a sharply demarcated, raised skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions lesion, with erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion, edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema, and warmth.
Necrotizing fasciitisNecrotizing fasciitisNecrotizing fasciitis is a life-threatening infection that causes rapid destruction and necrosis of the fascia and subcutaneous tissues. Patients may present with significant pain out of proportion to the presenting symptoms and rapidly progressive erythema of the affected area. Necrotizing Fasciitis: a rapidly progressive infection resulting in extensive necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage of subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess, fasciaFasciaLayers of connective tissue of variable thickness. The superficial fascia is found immediately below the skin; the deep fascia invests muscles, nerves, and other organs.Cellulitis, and muscle: Necrotizing fasciitisNecrotizing fasciitisNecrotizing fasciitis is a life-threatening infection that causes rapid destruction and necrosis of the fascia and subcutaneous tissues. Patients may present with significant pain out of proportion to the presenting symptoms and rapidly progressive erythema of the affected area. Necrotizing Fasciitis is most commonly caused by group A StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus but often involves other types of bacteriaBacteriaBacteria are prokaryotic single-celled microorganisms that are metabolically active and divide by binary fission. Some of these organisms play a significant role in the pathogenesis of diseases. Bacteriology in a mixed infection. The condition presents with necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, crepitusCrepitusOsteoarthritis, bullaeBullaeErythema Multiforme, and purple skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions discoloration.
DermatitisDermatitisAny inflammation of the skin.Atopic Dermatitis (Eczema): general term for edematous skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and FunctionsrashRashRocky Mountain Spotted Fever caused by an allergic reaction, irritant, or infection
Folliculitis: a localized inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the hair follicleHair follicleA tube-like invagination of the epidermis from which the hair shaft develops and into which sebaceous glands open. The hair follicle is lined by a cellular inner and outer root sheath of epidermal origin and is invested with a fibrous sheath derived from the dermis. Follicles of very long hairs extend into the subcutaneous layer of tissue under the skin.Cowden Syndrome or sebaceous glands that is primarily caused byS. aureusS. aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Staphylococcus: Presentation includes erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion, papules, pustules, and tenderness of the affected area.
ImpetigoImpetigoImpetigo is a highly contagious superficial bacterial infection typically caused by Staphylococcus aureus (most common) and Streptococcus pyogenes. Impetigo most commonly presents in children aged 2 to 5 years with lesions that evolve from papules to vesicles to pustules, which eventually break down to form characteristic “honey-colored” crusts. Impetigo: a highly contagious skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions infection of the upper epidermisEpidermisThe external, nonvascular layer of the skin. It is made up, from within outward, of five layers of epithelium: (1) basal layer (stratum basale epidermidis); (2) spinous layer (stratum spinosum epidermidis); (3) granular layer (stratum granulosum epidermidis); (4) clear layer (stratum lucidum epidermidis); and (5) horny layer (stratum corneum epidermidis).Skin: Structure and Functions: ImpetigoImpetigoImpetigo is a highly contagious superficial bacterial infection typically caused by Staphylococcus aureus (most common) and Streptococcus pyogenes. Impetigo most commonly presents in children aged 2 to 5 years with lesions that evolve from papules to vesicles to pustules, which eventually break down to form characteristic “honey-colored” crusts. Impetigo commonly affects children < 5 years of age and is caused by S. aureusS. aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Staphylococcus or group A StreptococcusStreptococcusStreptococcus is one of the two medically important genera of gram-positive cocci, the other being Staphylococcus. Streptococci are identified as different species on blood agar on the basis of their hemolytic pattern and sensitivity to optochin and bacitracin. There are many pathogenic species of streptococci, including S. pyogenes, S. agalactiae, S. pneumoniae, and the viridans streptococci.Streptococcus. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with an erythematous area covered in small vesiclesVesiclesFemale Genitourinary Examination, pustules, and/or honey-colored crusts.
Staphylococcal scalded skin syndromeStaphylococcal Scalded Skin SyndromeStaphylococcal scalded skin syndrome (SSSS), also known as Ritter disease and staphylococcal epidermal necrolysis, is a toxin-mediated condition caused by Staphylococcus aureus. The exfoliative toxin produced disseminates and cleaves desmoglein 1 in the epidermis, causing separation and detachment of the skin. Staphylococcal Scalded Skin Syndrome (SSSS): a toxin-mediated blistering skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions disorder caused by S. aureusS. aureusPotentially pathogenic bacteria found in nasal membranes, skin, hair follicles, and perineum of warm-blooded animals. They may cause a wide range of infections and intoxications.Staphylococcus. Presentation includes diffuse cutaneous erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion, tenderness, bullaeBullaeErythema Multiforme formation, and superficial desquamationDesquamationStaphylococcal Scalded Skin Syndrome (SSSS) (sloughing off of the superficial layer of skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions, leaving a red “scalded” appearance). The mucous membranes are spared.
Billing and Coding
Diagnosis Codes:
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis, a bacterial infection of the deeper layers of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions, is coded based on its anatomical location. It is crucial to specify the site for accurate documentationDocumentationSystematic organization, storage, retrieval, and dissemination of specialized information, especially of a scientific or technical nature. It often involves authenticating or validating information.Advance Directives.
Coding System
Code
Description
ICD-10-CM
L03.115
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis of right handHandThe hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. It consists of 5 metacarpal bones and 14 phalanges, as well as numerous muscles innervated by the median and ulnar nerves. Hand: Anatomy
ICD-10-CM
L03.116
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis of left lower legLegThe lower leg, or just “leg” in anatomical terms, is the part of the lower limb between the knee and the ankle joint. The bony structure is composed of the tibia and fibula bones, and the muscles of the leg are grouped into the anterior, lateral, and posterior compartments by extensions of fascia.Leg: Anatomy
ICD-10-CM
L03.90
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis, unspecified
Procedures/Interventions:
This code is for an incision and drainageIncision And DrainageChalazion (I&D), a procedure performed if the cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis is complicated by the formation of a distinct abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease.
Coding System
Code
Description
CPT
10060
Incision and drainageIncision And DrainageChalazion of abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease (eg, carbuncleCarbuncleInfectious Folliculitis, suppurative hidradenitis, cutaneous or subcutaneous abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease, cyst, furuncleFuruncleA purulent nodule arising from folliculitis that affects deeper layers of skin, including subcutaneous tissueInfectious Folliculitis, or paronychia); simple or single
Medications:
These codes are for oral antibiotics commonly used to treat uncomplicated cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis, such as cephalexin or clindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides, chosen based on likely pathogens and local resistanceResistancePhysiologically, the opposition to flow of air caused by the forces of friction. As a part of pulmonary function testing, it is the ratio of driving pressure to the rate of air flow.Ventilation: Mechanics of Breathing.
Coding System
Code
Description
RxNorm
2244
Cephalexin (ingredient)
RxNorm
2592
ClindamycinClindamycinAn antibacterial agent that is a semisynthetic analog of lincomycin.Lincosamides (ingredient)
Complications:
This code is for sepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, a life-threatening complication that can occur if the cellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis infection spreads into the bloodstream, leading to a systemic inflammatory response.
Coding System
Code
Description
ICD-10-CM
A41.9
SepsisSepsisSystemic inflammatory response syndrome with a proven or suspected infectious etiology. When sepsis is associated with organ dysfunction distant from the site of infection, it is called severe sepsis. When sepsis is accompanied by hypotension despite adequate fluid infusion, it is called septic shock.Sepsis and Septic Shock, unspecified organism
Ramakrishnan, K., Salinas, R. C., Agudelo Higuita, N. I. (2015). Skin and soft tissue infections. American Family Physician, 92(6), 474–483.
Klotz, C., et al. (2019). Adherence to antibiotic guidelines for erysipelas or cellulitis is associated with a favorable outcome. European Journal of Clinical Microbiology and Infectious Diseases, 38(4),703–709.
Stevens, D. L., et al. (2014). Executive summary: practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), 147–159. https://doi.org/10.1093/cid/ciu444
Alexiou, A., Narayanan, R. (2022). Cellulitis and erysipelas: symptoms, diagnosis, and treatment. BMJ Best Practice. Retrieved December 15, 2022, from https://bestpractice.bmj.com/topics/en-gb/3000172
Create your free account or log in to continue reading!