AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema occurring in the deep layers of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilationVasodilationThe physiological widening of blood vessels by relaxing the underlying vascular smooth muscle.Pulmonary Hypertension Drugs and increased capillary permeability. Clinically, angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema presents with swellingSwellingInflammation around the eyes, lipsLipsThe lips are the soft and movable most external parts of the oral cavity. The blood supply of the lips originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy, tongueTongueThe tongue, on the other hand, is a complex muscular structure that permits tasting and facilitates the process of mastication and communication. The blood supply of the tongue originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy, mouth, bowel wall, extremities, or genitalia. AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema may also compromise the airwayAirwayABCDE Assessment. UrticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives) will be present when the angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is mediated by mast cellsMast cellsGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Innate Immunity: Phagocytes and Antigen Presentation, but not when it is due to increases in bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency). Diagnosis is usually clinical but additional testing may include skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions/serum testing for specific antigens and C4 level assessment. Management depends on the underlying mechanism but may include treatment for anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction, removing any offending agents, antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines, glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids, and/or therapies that target bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency).
AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema occurring in the deep layers of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions and mucosal tissue.
May occur with or without urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives):
With urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives): indicates an IgE-mediated type I hypersensitivity reactionType I hypersensitivity reactionType I hypersensitivity reaction is an abnormal immune response triggered by exposure to specific antigens known as allergens. In this type of hypersensitivity reaction, the presentation of the antigen to the T-helper cells (Th cells) initiates a cascade of immunologic events leading to the production of antigen-specific IgE antibodies.Type I Hypersensitivity Reaction
Without urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives): mediated by substances other than IgEIgEAn immunoglobulin associated with mast cells. Overexpression has been associated with allergic hypersensitivity.Immunoglobulins: Types and Functions, usually bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)
Acute or chronic:
Acute angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema: < 6 weeks’ duration
Chronic angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema: 2–3 episodes per week for ≥ 6 weeks’ duration
Epidemiology[2,8,10]
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency:
Data on overall incidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency are limited.
Relatively common
Occurs in 40%–50% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with chronic urticariaChronic urticariaWheals and/or angioedema presented with daily symptoms lasting for more than 6 weeks. It may be classified into chronic spontaneous and chronic inducible urticaria depending on whether a specific trigger can be linked to the development of vascular reaction.Urticaria (Hives)
Approximately 10%–20% of people will experience an episode of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema at some point.
Age range:
Occurs in any age group
↑ IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency after adolescence (highest at 20–30 years old)
No genderGenderGender DysphoriabiasBiasEpidemiological studies are designed to evaluate a hypothesized relationship between an exposure and an outcome; however, the existence and/or magnitude of these relationships may be erroneously affected by the design and execution of the study itself or by conscious or unconscious errors perpetrated by the investigators or the subjects. These systematic errors are called biases. Types of Biases
AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema may result from 3 primary mechanisms:
Mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema–mediatedangioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema(most common and associated with urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives)):
Mast cellsMast cellsGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Innate Immunity: Phagocytes and Antigen Presentation are activated by:
IgEIgEAn immunoglobulin associated with mast cells. Overexpression has been associated with allergic hypersensitivity.Immunoglobulins: Types and Functions to specific antigens
Physical stimuliPhysical stimuliAct of eliciting a response from a person or organism through physical contact.Angioedema
Medications (non–IgE-mediated direct activation of mast cellsMast cellsGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Innate Immunity: Phagocytes and Antigen Presentation)
Once activated, mast cellsMast cellsGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Innate Immunity: Phagocytes and Antigen Presentation release inflammatory mediators:
Histamine
LeukotrienesLeukotrienesA family of biologically active compounds derived from arachidonic acid by oxidative metabolism through the 5-lipoxygenase pathway. They participate in host defense reactions and pathophysiological conditions such as immediate hypersensitivity and inflammation. They have potent actions on many essential organs and systems, including the cardiovascular, pulmonary, and central nervous system as well as the gastrointestinal tract and the immune system.Eicosanoids
ProstaglandinsProstaglandinsA group of compounds derived from unsaturated 20-carbon fatty acids, primarily arachidonic acid, via the cyclooxygenase pathway. They are extremely potent mediators of a diverse group of physiological processes.Eicosanoids
Heparin
Bradykinin-mediated angioedemaBradykinin-Mediated AngioedemaAngioedema(not associated with urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives)):
BradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) is an inflammatory mediator that can lead to vasodilationVasodilationThe physiological widening of blood vessels by relaxing the underlying vascular smooth muscle.Pulmonary Hypertension Drugs and vascular permeability.
↑ BradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) → ↑ vasodilationVasodilationThe physiological widening of blood vessels by relaxing the underlying vascular smooth muscle.Pulmonary Hypertension Drugs and ↑ vascular permeability
Due to:
↓ C1 inhibitorC1 inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Angioedema → ↓ inhibition of kinin generation → ↑ bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)
↑ Angiotensin-converting enzyme (ACE) inhibition → ↓ bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) degradation → ↑ bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)
Inflammatory mediators → ↑ vascular permeability and dilation of capillariesCapillariesCapillaries are the primary structures in the circulatory system that allow the exchange of gas, nutrients, and other materials between the blood and the extracellular fluid (ECF). Capillaries are the smallest of the blood vessels. Because a capillary diameter is so small, only 1 RBC may pass through at a time.Capillaries: Histology and venulesVenulesThe minute vessels that collect blood from the capillary plexuses and join together to form veins.Veins: Histology
Extravasation of fluid from vasculature → asymmetric edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema in the subcutaneous tissueSubcutaneous tissueLoose connective tissue lying under the dermis, which binds skin loosely to subjacent tissues. It may contain a pad of adipocytes, which vary in number according to the area of the body and vary in size according to the nutritional state.Soft Tissue Abscess and deep dermisDeep DermisErysipelas:
Occurs in areas of affected vasculature
Not gravitationally dependent
Mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema–mediated etiologies[2,11]
Mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema–mediated angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is typically associated with urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives).
IgEIgEAn immunoglobulin associated with mast cells. Overexpression has been associated with allergic hypersensitivity.Immunoglobulins: Types and Functions to specific antigens (type I hypersensitivity reactions):
Insect stingsInsect stingsInsect and scorpion stings are a rare cause of mortality. Hymenoptera insects and Centruroides scorpions can potentially lead to serious symptoms due to envenomation. Pain, swelling, erythema, and warmth are common at the site of a sting. Insect and Scorpion Stings (venom) and bites
Latex
Physical stimuliPhysical stimuliAct of eliciting a response from a person or organism through physical contact.Angioedema:
Medications (directly stimulate mast cellsMast cellsGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Innate Immunity: Phagocytes and Antigen Presentation without IgEIgEAn immunoglobulin associated with mast cells. Overexpression has been associated with allergic hypersensitivity.Immunoglobulins: Types and Functions):
OpioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics
Most commonly due to aspirinAspirinThe prototypical analgesic used in the treatment of mild to moderate pain. It has anti-inflammatory and antipyretic properties and acts as an inhibitor of cyclooxygenase which results in the inhibition of the biosynthesis of prostaglandins. Aspirin also inhibits platelet aggregation and is used in the prevention of arterial and venous thrombosis.Nonsteroidal Antiinflammatory Drugs (NSAIDs)
Note: IgE-mediated allergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction and direct mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema stimulation are both possible.
Radiocontrast agents
Bradykinin-mediated etiologies[2,4,8]
These etiologies are not associated with histamine release or urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives).
Dysfunctional C1 inhibitorC1 inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Angioedema:
Hereditary angioedemaHereditary angioedemaForms of hereditary angioedema that occur due to mutations in the gene for complement C1 inhibitor protein. Type I hereditary angioedema is associated with reduced serum levels of complement C1 inhibitor protein. Type II hereditary angioedema is associated with the production of a non-functional complement C1 inhibitor protein.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) (HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency); an autosomal dominantAutosomal dominantAutosomal inheritance, both dominant and recessive, refers to the transmission of genes from the 22 autosomal chromosomes. Autosomal dominant diseases are expressed when only 1 copy of the dominant allele is inherited. Autosomal Recessive and Autosomal Dominant Inheritance abnormality in the quantity or function of C1 inhibitorC1 inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Angioedema (C1 INH)):[11,13,14]
HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)type 1Type 1Spinal Muscular Atrophy (85% of cases): ↓ production of functionally active C1 INH
HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) type 2: normal levels of C1 INH but functionally impaired protein
HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)type 3Type 3Spinal Muscular Atrophy: mutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations in coagulation factor XII (normal C1 INH level and function); more commonly seen in women
Acquired C1 inhibitor deficiencyC1 inhibitor deficiencyForms of hereditary angioedema that occur due to mutations in the gene for complement C1 inhibitor protein. Type I hereditary angioedema is associated with reduced serum levels of complement C1 inhibitor protein. Type II hereditary angioedema is associated with the production of a non-functional complement C1 inhibitor protein.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema (development of antibodiesAntibodiesImmunoglobulins (Igs), also known as antibodies, are glycoprotein molecules produced by plasma cells that act in immune responses by recognizing and binding particular antigens. The various Ig classes are IgG (the most abundant), IgM, IgE, IgD, and IgA, which differ in their biologic features, structure, target specificity, and distribution.Immunoglobulins: Types and Functions against C1 inhibitorC1 inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Angioedema):[12]
Very rare
Majority of cases are diagnosed at ≥ 40 years of age.
Often associated with lymphoproliferative disordersLymphoproliferative disordersDisorders characterized by proliferation of lymphoid tissue, general or unspecified.Lymphocytosis
Medications (both via ↓ bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) degradation):
ACE inhibitorsACE inhibitorsTruncus Arteriosus (ACEisACEIsA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Heart Failure and Chronic Coronary Syndrome Medication)
Dipeptidyl peptidase-4Dipeptidyl peptidase-4A serine protease that catalyses the release of an n-terminal dipeptide. Several biologically-active peptides have been identified as dipeptidyl peptidase 4 substrates including incretins; neuropeptides; and chemokines. The protein is also found bound to adenosine deaminase on the t-cell surface and is believed to play a role in t-cell activation.Angioedema inhibitors
Other etiologies[2]
UrticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives) may or may not be present.
IdiopathicIdiopathicDermatomyositisangioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema:
An etiology is not determined after a thorough evaluation.
Commonly associated with chronic angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema
Other causes of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema with unknown mechanisms:
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease:
Common coldCommon coldA catarrhal disorder of the upper respiratory tract, which may be viral or a mixed infection. It generally involves a runny nose, nasal congestion, and sneezing.Rhinovirus
Urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes channel blockers
AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema presents in various ways, depending on the site(s) and mechanism involved.[3,6,11]
LipsLipsThe lips are the soft and movable most external parts of the oral cavity. The blood supply of the lips originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy, mouth, tongueTongueThe tongue, on the other hand, is a complex muscular structure that permits tasting and facilitates the process of mastication and communication. The blood supply of the tongue originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy
ThroatThroatThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking.Pharynx: Anatomy, larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy, and uvulaUvulaA fleshy extension at the back of the soft palate that hangs above the opening of the throat.Peritonsillar Abscess
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
Mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema–mediated: minutes to hours
Bradykinin-mediated: hours to days
Spontaneous resolution (hours to days)
Asymmetric distribution
Form in nongravitationally dependent areas
UrticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives) (in mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema–mediated cases only)
AnaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction:
Life-threatening throatThroatThe pharynx is a component of the digestive system that lies posterior to the nasal cavity, oral cavity, and larynx. The pharynx can be divided into the oropharynx, nasopharynx, and laryngopharynx. Pharyngeal muscles play an integral role in vital processes such as breathing, swallowing, and speaking.Pharynx: Anatomy and airwayAirwayABCDE AssessmentswellingSwellingInflammation → impaired airflow
Signs and symptoms:
Shortness of breathShortness of breathDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary).Dyspnea
WheezingWheezingWheezing is an abnormal breath sound characterized by a whistling noise that can be relatively high-pitched and shrill (more common) or coarse. Wheezing is produced by the movement of air through narrowed or compressed small (intrathoracic) airways. Wheezing and stridorStridorLaryngomalacia and Tracheomalacia
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension
Table: Clinical features of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema[10,12]
Histamine-mediated
Bradykinin-mediated
Onset
Rapid onset (minutes to hours)
Hours to days
Duration
12–24 hours
48–72 hours
Head and neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess
presentation
Lip/tongueTongueThe tongue, on the other hand, is a complex muscular structure that permits tasting and facilitates the process of mastication and communication. The blood supply of the tongue originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: AnatomyswellingSwellingInflammation
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension/shockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock
WheezingWheezingWheezing is an abnormal breath sound characterized by a whistling noise that can be relatively high-pitched and shrill (more common) or coarse. Wheezing is produced by the movement of air through narrowed or compressed small (intrathoracic) airways. Wheezing/bronchospasmBronchospasmAsthma Drugs
Atypical
Dermatologic presentation
UrticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives) PruritusPruritusAn intense itching sensation that produces the urge to rub or scratch the skin to obtain relief.Atopic Dermatitis (Eczema)
Atypical
Abdominal presentation
Abdominal painAbdominal PainAcute Abdomen + NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Abdominal painAbdominal PainAcute Abdomen ++ NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
Abdominal swellingSwellingInflammation
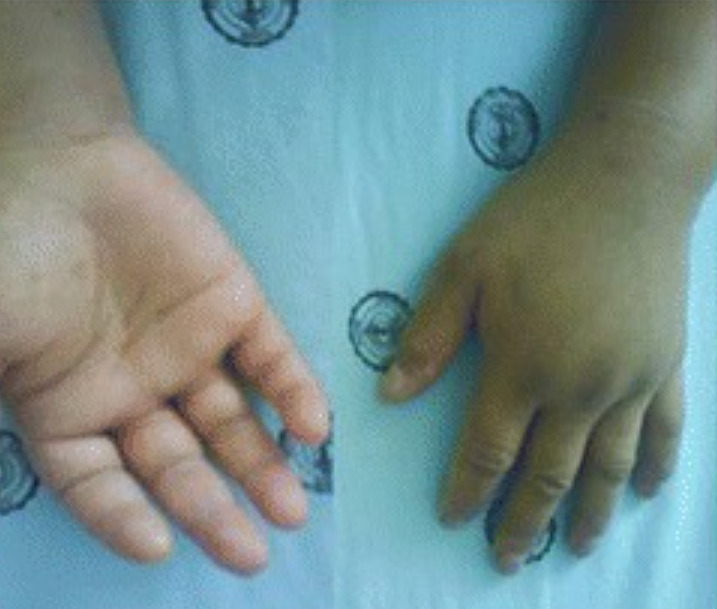
Significant swelling of the hands due to angioedema
Image: “Acute adult-onset Still’s disease presenting as pulmonary hemorrhage, urticaria, angioedema, and leukemoid reaction: a case report and literature review” by Mora Alfonso SA, Rodríguez DM, Londoño JD, Valle-Oñate R, Quintana G. License: CC BY 4.0, edited by Lecturio.
Asymmetrical swelling of the face and lips due to angioedema
Image: “Angioedema of the face” by Boussetta et al. License: CC BY 4.0
Diagnosis
The diagnosis of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is usually clinical, but testing can help to clarify the etiology. Most cases of chronic angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema are idiopathicIdiopathicDermatomyositis.[3,4,6,11]
Associated urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives)
Any past episodes
Coexisting medical conditions:
AllergiesAllergiesA medical specialty concerned with the hypersensitivity of the individual to foreign substances and protection from the resultant infection or disorder.Selective IgA Deficiency
Autoimmune conditions
Gastrointestinal symptoms (swellingSwellingInflammation of the lining of the intestinal tracts can cause painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways/cramping)
Family historyFamily HistoryAdult Health Maintenance of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema
Mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema–mediated angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema with urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives):
With anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction: ↑ tryptaseTryptaseA family of neutral serine proteases with trypsin-like activity. Tryptases are primarily found in the secretory granules of mast cells and are released during mast cell degranulation.Exocrine Pancreatic Cancer confirms mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema activation
AllergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity ReactionskinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions testing
Medication withdrawal and challenge
Repeat physical stimuliPhysical stimuliAct of eliciting a response from a person or organism through physical contact.Angioedema (if suspected as triggering event).
Serum IgE antibodiesIgE antibodiesAn immunoglobulin associated with mast cells. Overexpression has been associated with allergic hypersensitivity.Type I Hypersensitivity Reaction to specific antigens
Isolated angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema without urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives):
↑ CRP → infection, ACEI-induced angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema
↓ Complement protein C4 → evaluate for HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) or acquired C1 inhibitor deficiencyC1 inhibitor deficiencyForms of hereditary angioedema that occur due to mutations in the gene for complement C1 inhibitor protein. Type I hereditary angioedema is associated with reduced serum levels of complement C1 inhibitor protein. Type II hereditary angioedema is associated with the production of a non-functional complement C1 inhibitor protein.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency):
C1 inhibitorC1 inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.AngioedemaantigenAntigenSubstances that are recognized by the immune system and induce an immune reaction.Vaccination/concentration
C1 inhibitorC1 inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Angioedema function levels
Note that results on C4 and C1 INH will not be available in the ED, but should be followed up in the outpatient setting.
Suspect HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency):[14]
When presentation includes:
Recurrent angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema without urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives)
Family historyFamily HistoryAdult Health Maintenance of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema
When C4 and C1 INH are decreased, repeat the test to confirm.
Normal C4 rules out HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) types 1 and 2.
Early age at onset suggests type 1Type 1Spinal Muscular AtrophyHAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) (most cases present before age 15).
Later age at onset suggests acquired angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema.
Genetic testingGenetic TestingDetection of a mutation; genotype; karyotype; or specific alleles associated with genetic traits, heritable diseases, or predisposition to a disease, or that may lead to the disease in descendants. It includes prenatal genetic testing.Myotonic Dystrophies (mutations in C1 INH geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics (SERPING1geneGeneA category of nucleic acid sequences that function as units of heredity and which code for the basic instructions for the development, reproduction, and maintenance of organisms.Basic Terms of Genetics)):[13]
Can be useful in confirming the diagnosis in those < 1 year of age
Table: Diagnostic testsDiagnostic testsDiagnostic tests are important aspects in making a diagnosis. Some of the most important epidemiological values of diagnostic tests include sensitivity and specificity, false positives and false negatives, positive and negative predictive values, likelihood ratios, and pre-test and post-test probabilities. Epidemiological Values of Diagnostic Tests in angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema[12]
C1 INH concentration
C1 INH function
C4 concentration
TryptaseTryptaseA family of neutral serine proteases with trypsin-like activity. Tryptases are primarily found in the secretory granules of mast cells and are released during mast cell degranulation.Exocrine Pancreatic Cancer concentration*
HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)type 1Type 1Spinal Muscular Atrophy
Low
Low
Low
Normal
HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) type 2
Normal/high
Low
Low
Normal
HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)type 3Type 3Spinal Muscular Atrophy
Normal
Normal
Normal
Normal
Acquired (C1 INH deficiency) angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema
Low
Low
Low
Normal
ACEi-induced angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema
Normal
Normal
Normal
Normal
Histamine-mediated anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction
Normal
Normal
Normal
Normal/elevated
*Drawn within 4–6 hours after onset
Management
Management guidelines may vary depending on practice location. The following information is based on US and UK literature and guidelines.
In general, if angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema affects the area anterior to the teethTeethNormally, an adult has 32 teeth: 16 maxillary and 16 mandibular. These teeth are divided into 4 quadrants with 8 teeth each. Each quadrant consists of 2 incisors (dentes incisivi), 1 canine (dens caninus), 2 premolars (dentes premolares), and 3 molars (dentes molares). Teeth are composed of enamel, dentin, and dental cement.Teeth: Anatomy (e.g., lipsLipsThe lips are the soft and movable most external parts of the oral cavity. The blood supply of the lips originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy), intubationIntubationPeritonsillar Abscess is not needed.
Prepare for cricothyrotomyCricothyrotomyABCDE Assessment (double setup) before attempting intubationIntubationPeritonsillar Abscess (in case endotracheal intubationIntubationPeritonsillar Abscess is not possible with severe edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema).
Assess for anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction → stabilize if present:[10]
EpinephrineEpinephrineThe active sympathomimetic hormone from the adrenal medulla. It stimulates both the alpha- and beta- adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels.Sympathomimetic Drugs 0.3–0.5 mg IM (using 1 mg/mL solution); repeat dosing if symptoms persist or return.
Intravenous fluidsIntravenous FluidsIntravenous fluids are one of the most common interventions administered in medicine to approximate physiologic bodily fluids. Intravenous fluids are divided into 2 categories: crystalloid and colloid solutions. Intravenous fluids have a wide variety of indications, including intravascular volume expansion, electrolyte manipulation, and maintenance fluids. Intravenous Fluids
Oxygen
Discontinue any potential causative medications.
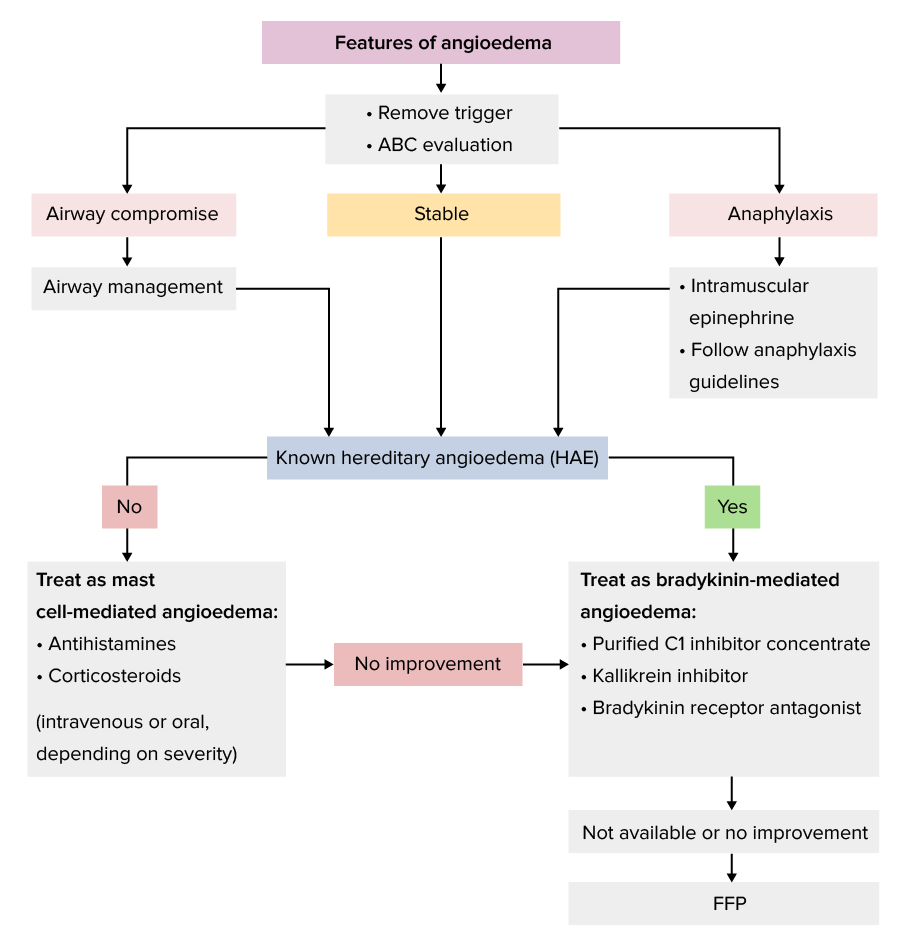
Algorithm for the management of angioedema in the acute setting.[10–12]
Image by Lecturio.
Management of mast cellMast cellGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Angioedema–mediated angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema[10–12]
General approach for non-anaphylactic presentation:
Identify and remove triggers.
For people with mild symptoms, treatment may not be needed.[9]
Main treatment involves antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines and glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids.
H1 antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines (1st line): to suppress histamine released by mast cellsMast cellsGranulated cells that are found in almost all tissues, most abundantly in the skin and the gastrointestinal tract. Like the basophils, mast cells contain large amounts of histamine and heparin. Unlike basophils, mast cells normally remain in the tissues and do not circulate in the blood. Mast cells, derived from the bone marrow stem cells, are regulated by the stem cell factor.Innate Immunity: Phagocytes and Antigen Presentation:
DiphenhydramineDiphenhydramineA histamine h1 antagonist used as an antiemetic, antitussive, for dermatoses and pruritus, for hypersensitivity reactions, as a hypnotic, an antiparkinson, and as an ingredient in common cold preparations. It has some undesired antimuscarinic and sedative effects.Antihistamines:
10–50 mg IV (for time-critical treatment)
25–50 mg orally every 6 hours as needed
ChlorpheniramineChlorpheniramineA histamine h1 antagonist used in allergic reactions, hay fever, rhinitis, urticaria, and asthma. It has also been used in veterinary applications. One of the most widely used of the classical antihistaminics, it generally causes less drowsiness and sedation than promethazine.Antihistamines (UK): 10–20 mg IV (for time-critical treatment)
CetirizineCetirizineA potent second-generation histamine h1 antagonist that is effective in the treatment of allergic rhinitis, chronic urticaria, and pollen-induced asthma. Unlike many traditional antihistamines, it does not cause drowsiness or anticholinergic side effects.Antihistamines 10–20 mg orally twice a day
LoratadineLoratadineA second-generation histamine h1 receptor antagonist used in the treatment of allergic rhinitis and urticaria. Unlike most classical antihistamines (histamine h1 antagonists) it lacks central nervous system depressing effects such as drowsiness.Antihistamines 10 mg orally daily
Addition of H2 antagonists helps relieve urticariaUrticariaUrticaria is raised, well-circumscribed areas (wheals) of edema (swelling) and erythema (redness) involving the dermis and epidermis with associated pruritus (itch). Urticaria is not a single disease but rather is a reaction pattern representing cutaneous mast cell degranulation.Urticaria (Hives) (if present); H2 receptorsH2 ReceptorsAntihistamines comprise about 15% of cutaneous histamine receptorsHistamine ReceptorsAntihistamines.
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants 20–40 mg/day orally (tapered over 5–7 days)
PrednisolonePrednisoloneA glucocorticoid with the general properties of the corticosteroids. It is the drug of choice for all conditions in which routine systemic corticosteroid therapy is indicated, except adrenal deficiency states.Immunosuppressants 0.5–1 mg/kg/day (over 5–7 days)
Rapidly developing angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema without anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction:
IV antihistamine (diphenhydramineDiphenhydramineA histamine h1 antagonist used as an antiemetic, antitussive, for dermatoses and pruritus, for hypersensitivity reactions, as a hypnotic, an antiparkinson, and as an ingredient in common cold preparations. It has some undesired antimuscarinic and sedative effects.Antihistamines; chlorphenamine also available in UK)
Approach angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema involving the neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess, face, tongueTongueThe tongue, on the other hand, is a complex muscular structure that permits tasting and facilitates the process of mastication and communication. The blood supply of the tongue originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy, and/or lipsLipsThe lips are the soft and movable most external parts of the oral cavity. The blood supply of the lips originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy as potentially life-threatening.
Observe for at least 2–6 hours, as necessary, to ensure that symptoms are resolving and that no airwayAirwayABCDE Assessment obstruction is developing.
May require longer observation and have a low thresholdThresholdMinimum voltage necessary to generate an action potential (an all-or-none response)Skeletal Muscle Contraction for admission (Severe acute angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema can have a late-phase reaction.)
Stable angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema without anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction:
Oral antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines (up to 6 weeks)
Additional short course of oral glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids
Observe for at least 2–6 hours, as necessary, to ensure that symptoms are resolving and that no airwayAirwayABCDE Assessment obstruction is developing.
1st-line options to attempt to ↓ bradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency):
Purified C1 inhibitorC1 inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Angioedema concentrate
KallikreinKallikreinProteolytic enzymes from the serine endopeptidase family found in normal blood and urine. Specifically, kallikreins are potent vasodilators and hypotensives and increase vascular permeability and affect smooth muscle. They act as infertility agents in men. Three forms are recognized, plasma kallikrein, tissue kallikrein, and prostate-specific antigen.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) inhibitor: ecallantide
≥ 12 years of age: 30 mg SC once (away from site of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema)
May repeat dose once within 24 hours.
BradykininBradykininA nonapeptide messenger that is enzymatically produced from kallidin in the blood where it is a potent but short-lived agent of arteriolar dilation and increased capillary permeability. Bradykinin is also released from mast cells during asthma attacks, from gut walls as a gastrointestinal vasodilator, from damaged tissues as a pain signal, and may be a neurotransmitter.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) B2 receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonist: icatibant acetate
Worsening HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)
Use of epinephrineEpinephrineThe active sympathomimetic hormone from the adrenal medulla. It stimulates both the alpha- and beta- adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels.Sympathomimetic Drugs, glucocorticoidsGlucocorticoidsGlucocorticoids are a class within the corticosteroid family. Glucocorticoids are chemically and functionally similar to endogenous cortisol. There are a wide array of indications, which primarily benefit from the antiinflammatory and immunosuppressive effects of this class of drugs.Glucocorticoids, and antihistamine:
Although HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) is unlikely to respond, these medications are not contraindicated.
If the cause of the angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is not known, administer these medications.
Analgesics and antiemeticsAntiemeticsAntiemetics are medications used to treat and/or prevent nausea and vomiting. These drugs act on different target receptors. The main classes include benzodiazepines, corticosteroids, atypical antipsychotics, cannabinoids, and antagonists of the following receptors: serotonin, dopamine, and muscarinic and neurokinin receptors.Antiemetics as needed
ACEi-associated angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema:
The above therapies for HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) can be used, but their efficacy has not been proven.
Most cases resolve 24–72 hours after discontinuing the ACEiACEiA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Renin-Angiotensin-Aldosterone System Inhibitors.
Management of chronic idiopathicIdiopathicDermatomyositisangioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema[10,11]
PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship should be referred to an allergyAllergyAn abnormal adaptive immune response that may or may not involve antigen-specific IgEType I Hypersensitivity Reaction specialist.
Medical therapy:
Nonsedating antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines:
CetirizineCetirizineA potent second-generation histamine h1 antagonist that is effective in the treatment of allergic rhinitis, chronic urticaria, and pollen-induced asthma. Unlike many traditional antihistamines, it does not cause drowsiness or anticholinergic side effects.Antihistamines
LoratadineLoratadineA second-generation histamine h1 receptor antagonist used in the treatment of allergic rhinitis and urticaria. Unlike most classical antihistamines (histamine h1 antagonists) it lacks central nervous system depressing effects such as drowsiness.Antihistamines
LeukotrieneLeukotrieneAsthma DrugsreceptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors antagonist (montelukastMontelukastAsthma Drugs) can be added.
For acute episodes:
PrednisonePrednisoneA synthetic anti-inflammatory glucocorticoid derived from cortisone. It is biologically inert and converted to prednisolone in the liver.Immunosuppressants
DiphenhydramineDiphenhydramineA histamine h1 antagonist used as an antiemetic, antitussive, for dermatoses and pruritus, for hypersensitivity reactions, as a hypnotic, an antiparkinson, and as an ingredient in common cold preparations. It has some undesired antimuscarinic and sedative effects.Antihistamines
Additional treatment considerations[9,12]
Admit patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship in the following cases:
AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema with anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction
Rapidly developing angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema
Worsening of symptoms or no improvement with treatment
Worsening symptoms may be cutaneous (increased swellingSwellingInflammation) or development of other features (abdominal painAbdominal PainAcute Abdomen, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, rhinitisRhinitisInflammation of the nasal mucosa, the mucous membrane lining the nasal cavities.Rhinitis).
Ensure that the patient is seen by the primary care physician or medical team after discharge in order to:
Check for continued improvement or resolution of symptoms
Follow up on test results
Proceed with further workup or referrals, as indicated
Refer to a dermatologist or immunologist if:
Hereditary or acquired angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is suspected.
Symptoms persist or recur 3 months after stopping treatment with an ACEiACEiA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Renin-Angiotensin-Aldosterone System Inhibitors.
The cause of the angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema is neither identifiable nor avoidable.
For people awaiting specialist review who are at risk for anaphylaxisAnaphylaxisAn acute hypersensitivity reaction due to exposure to a previously encountered antigen. The reaction may include rapidly progressing urticaria, respiratory distress, vascular collapse, systemic shock, and death.Type I Hypersensitivity Reaction:
Prescribe epinephrineEpinephrineThe active sympathomimetic hormone from the adrenal medulla. It stimulates both the alpha- and beta- adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels.Sympathomimetic Drugs auto-injector. (Consider discontinuation of concomitant beta-blocker medication, which can interfere with its actions.)
High-risk individuals include those with:
AsthmaAsthmaAsthma is a chronic inflammatory respiratory condition characterized by bronchial hyperresponsiveness and airflow obstruction. The disease is believed to result from the complex interaction of host and environmental factors that increase disease predisposition, with inflammation causing symptoms and structural changes. Patients typically present with wheezing, cough, and dyspnea. Asthma
AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema triggered by trace amounts of allergen
AngioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema caused by an unavoidable triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical Ventilation
For those who experienced life-threatening angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema, avoid ACEiACEiA class of drugs whose main indications are the treatment of hypertension and heart failure. They exert their hemodynamic effect mainly by inhibiting the renin-angiotensin system. They also modulate sympathetic nervous system activity and increase prostaglandin synthesis. They cause mainly vasodilation and mild natriuresis without affecting heart rate and contractility.Renin-Angiotensin-Aldosterone System Inhibitors and angiotensin receptorReceptorReceptors are proteins located either on the surface of or within a cell that can bind to signaling molecules known as ligands (e.g., hormones) and cause some type of response within the cell.Receptors blockers.
Additionally, avoid hormone replacement therapyHormone Replacement TherapyHormone replacement therapy (HRT) is used to treat symptoms associated with female menopause and in combination to suppress ovulation. Risks and side effects include uterine bleeding, predisposition to cancer, breast tenderness, hyperpigmentation, migraine headaches, hypertension, bloating, and mood changes.Noncontraceptive Estrogen and Progestins and estrogenEstrogenCompounds that interact with estrogen receptors in target tissues to bring about the effects similar to those of estradiol. Estrogens stimulate the female reproductive organs, and the development of secondary female sex characteristics. Estrogenic chemicals include natural, synthetic, steroidal, or non-steroidal compounds.Ovaries: Anatomy contraceptives (which can triggerTriggerThe type of signal that initiates the inspiratory phase by the ventilatorInvasive Mechanical VentilationangioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema) in those with HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency).[14]
Differential Diagnosis
Contact dermatitisContact dermatitisA type of acute or chronic skin reaction in which sensitivity is manifested by reactivity to materials or substances coming in contact with the skin. It may involve allergic or non-allergic mechanisms.Male Genitourinary Examination: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions in response to contact irritants, which can affect the face in some circumstances (often cosmetics or topical pharmaceuticals). EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema and pruritusPruritusAn intense itching sensation that produces the urge to rub or scratch the skin to obtain relief.Atopic Dermatitis (Eczema) may develop mimicking angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema. Microvesiculation (formation of small vesiclesVesiclesFemale Genitourinary Examination), painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, and a burning sensation can help distinguish contact dermatitisContact dermatitisA type of acute or chronic skin reaction in which sensitivity is manifested by reactivity to materials or substances coming in contact with the skin. It may involve allergic or non-allergic mechanisms.Male Genitourinary Examination from angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema. Management involves removing the offending agent and reducing skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and FunctionsinflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation with steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors or topical calcineurin inhibitorsCalcineurin InhibitorsCompounds that inhibit or block the phosphatase activity of calcineurin.Immunosuppressants.
CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis and erysipelasErysipelasErysipelas is a bacterial infection of the superficial layer of the skin extending to the skin’s superficial lymphatic vessels. This infection presents as a raised, well-defined, tender, and bright red rash. Typically on the legs or face, but erysipelas can occur anywhere on the skin. Erysipelas: skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and FunctionsinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease presenting with well-demarcated erythemaErythemaRedness of the skin produced by congestion of the capillaries. This condition may result from a variety of disease processes.Chalazion, edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema, and warmth. CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis involves the deeper dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions and subcutaneous fatSubcutaneous fatFatty tissue under the skin throughout the body.Erythema Nodosum while erysipelasErysipelasErysipelas is a bacterial infection of the superficial layer of the skin extending to the skin’s superficial lymphatic vessels. This infection presents as a raised, well-defined, tender, and bright red rash. Typically on the legs or face, but erysipelas can occur anywhere on the skin. Erysipelas involves the upper dermisDermisA layer of vascularized connective tissue underneath the epidermis. The surface of the dermis contains innervated papillae. Embedded in or beneath the dermis are sweat glands; hair follicles; and sebaceous glands.Skin: Structure and Functions. CellulitisCellulitisCellulitis is a common infection caused by bacteria that affects the dermis and subcutaneous tissue of the skin. It is frequently caused by Staphylococcus aureus and Streptococcus pyogenes. The skin infection presents as an erythematous and edematous area with warmth and tenderness. Cellulitis and erysipelasErysipelasErysipelas is a bacterial infection of the superficial layer of the skin extending to the skin’s superficial lymphatic vessels. This infection presents as a raised, well-defined, tender, and bright red rash. Typically on the legs or face, but erysipelas can occur anywhere on the skin. Erysipelas tend to be accompanied by a feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, are more painful than angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema, and have more pronounced demarcation than angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema. The diagnosis is clinical, and management is with antibiotics.
Autoimmune conditions: systemic lupus erythematosusSystemic lupus erythematosusSystemic lupus erythematosus (SLE) is a chronic autoimmune, inflammatory condition that causes immune-complex deposition in organs, resulting in systemic manifestations. Women, particularly those of African American descent, are more commonly affected.Systemic Lupus Erythematosus, polymyositisPolymyositisPolymyositis (PM) is an autoimmune inflammatory myopathy caused by T cell-mediated muscle injury. The etiology of PM is unclear, but there are several genetic and environmental associations. Polymyositis is most common in middle-aged women and rarely affects children. Polymyositis, dermatomyositisDermatomyositisA subacute or chronic inflammatory disease of muscle and skin, marked by proximal muscle weakness and a characteristic skin rash. The illness occurs with approximately equal frequency in children and adults. The skin lesions usually take the form of a purplish rash (or less often an exfoliative dermatitis) involving the nose, cheeks, forehead, upper trunk, and arms. The disease is associated with a complement mediated intramuscular microangiopathy, leading to loss of capillaries, muscle ischemia, muscle-fiber necrosis, and perifascicular atrophy. The childhood form of this disease tends to evolve into a systemic vasculitis. Dermatomyositis may occur in association with malignant neoplasms.Paraneoplastic Syndromes, and Sjogren’s syndrome, which may all present with edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema of the face, periorbitalPeriorbitalOrbital and Preseptal Cellulitis areas, and hands. The presence of other findings (e.g., Raynaud’s phenomenon, dry eyes/mouth, and characteristic rashesRashesRashes are a group of diseases that cause abnormal coloration and texture to the skin. The etiologies are numerous but can include irritation, allergens, infections, or inflammatory conditions. Rashes that present in only 1 area of the body are called localized rashes. Generalized rashes occur diffusely throughout the body. Generalized and Localized Rashes) differentiates the autoimmune conditions from angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema. The diagnosis is based on clinical findings and antibody testing. Management varies but often includes steroidsSteroidsA group of polycyclic compounds closely related biochemically to terpenes. They include cholesterol, numerous hormones, precursors of certain vitamins, bile acids, alcohols (sterols), and certain natural drugs and poisons. Steroids have a common nucleus, a fused, reduced 17-carbon atom ring system, cyclopentanoperhydrophenanthrene. Most steroids also have two methyl groups and an aliphatic side-chain attached to the nucleus.Benign Liver Tumors and immunosuppressantsImmunosuppressantsImmunosuppressants are a class of drugs widely used in the management of autoimmune conditions and organ transplant rejection. The general effect is dampening of the immune response.Immunosuppressants.
Superior vena cavaSuperior vena cavaThe venous trunk which returns blood from the head, neck, upper extremities and chest.Mediastinum and Great Vessels: Anatomy (SVC) syndrome: tumors involving the right lung, lymph nodesLymph NodesThey are oval or bean shaped bodies (1 – 30 mm in diameter) located along the lymphatic system.Lymphatic Drainage System: Anatomy, or mediastinal structures that may obstruct blood flowBlood flowBlood flow refers to the movement of a certain volume of blood through the vasculature over a given unit of time (e.g., mL per minute).Vascular Resistance, Flow, and Mean Arterial Pressure through the SVC by direct invasion or external compressionExternal CompressionBlunt Chest Trauma, causing swellingSwellingInflammation in the face or neckNeckThe part of a human or animal body connecting the head to the rest of the body.Peritonsillar Abscess and dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea. Other symptoms (e.g., chest painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways, respiratory, or neurologic) help distinguish SVC syndrome from angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema. Diagnosis is with imaging and venographyVenographyBudd-Chiari Syndrome. Management involves treatment for the malignancyMalignancyHemothorax and techniques to relieve the obstruction.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema, a localized swellingSwellingInflammation of the deep layers of the skinSkinThe skin, also referred to as the integumentary system, is the largest organ of the body. The skin is primarily composed of the epidermis (outer layer) and dermis (deep layer). The epidermis is primarily composed of keratinocytes that undergo rapid turnover, while the dermis contains dense layers of connective tissue.Skin: Structure and Functions or mucous membranes. It is crucial to differentiate between allergic/idiopathicIdiopathicDermatomyositis forms and hereditary angioedemaHereditary angioedemaForms of hereditary angioedema that occur due to mutations in the gene for complement C1 inhibitor protein. Type I hereditary angioedema is associated with reduced serum levels of complement C1 inhibitor protein. Type II hereditary angioedema is associated with the production of a non-functional complement C1 inhibitor protein.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) (HAEHAEHereditary angioedema (HAE), also known as C1 esterase inhibitor (c1-inh) deficiency, is an autosomal dominant disorder characterized by recurrent episodes of severe swelling (angioedema). Hereditary angioedema commonly affects the limbs, face, intestinal tract, and upper airway.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency)).
Coding System
Code
Description
ICD-10-CM
T78.3XXA
Angioneurotic edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema, not elsewhere classified, initial encounter
ICD-10-CM
D84.1
Defect in the complement systemComplement systemSerum glycoproteins participating in the host defense mechanism of complement activation that creates the complement membrane attack complex. Included are glycoproteins in the various pathways of complement activation (classical complement pathway; alternative complement pathway; and lectin complement pathway).Innate Immunity: Barriers, Complement, and Cytokines (includes Hereditary AngioedemaHereditary angioedemaForms of hereditary angioedema that occur due to mutations in the gene for complement C1 inhibitor protein. Type I hereditary angioedema is associated with reduced serum levels of complement C1 inhibitor protein. Type II hereditary angioedema is associated with the production of a non-functional complement C1 inhibitor protein.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency))
Medications:
These codes represent treatments for angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema. EpinephrineEpinephrineThe active sympathomimetic hormone from the adrenal medulla. It stimulates both the alpha- and beta- adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels.Sympathomimetic Drugs and antihistaminesAntihistaminesAntihistamines are drugs that target histamine receptors, particularly H1 and H2 receptors. H1 antagonists are competitive and reversible inhibitors of H1 receptors. First-generation antihistamines cross the blood-brain barrier and can cause sedation. Antihistamines are used for allergic angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema, while C1 esterase inhibitorC1 esterase inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) is a specific therapy for hereditary angioedemaHereditary angioedemaForms of hereditary angioedema that occur due to mutations in the gene for complement C1 inhibitor protein. Type I hereditary angioedema is associated with reduced serum levels of complement C1 inhibitor protein. Type II hereditary angioedema is associated with the production of a non-functional complement C1 inhibitor protein.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency).
Coding System
Code
Description
RxNorm
3820
EpinephrineEpinephrineThe active sympathomimetic hormone from the adrenal medulla. It stimulates both the alpha- and beta- adrenergic systems, causes systemic vasoconstriction and gastrointestinal relaxation, stimulates the heart, and dilates bronchi and cerebral vessels.Sympathomimetic Drugs (ingredient)
RxNorm
3498
DiphenhydramineDiphenhydramineA histamine h1 antagonist used as an antiemetic, antitussive, for dermatoses and pruritus, for hypersensitivity reactions, as a hypnotic, an antiparkinson, and as an ingredient in common cold preparations. It has some undesired antimuscarinic and sedative effects.Antihistamines (ingredient)
RxNorm
1010048
C1 esterase inhibitorC1 esterase inhibitorAn endogenous 105-kda plasma glycoprotein produced primarily by the liver and monocytes. It inhibits a broad spectrum of proteases, including the complement C1r and the complement C1s proteases of the classical complement pathway, and the mannose-binding protein-associated serine proteases. C1-inh-deficient individuals suffer from hereditary angioedema types I and II.Hereditary Angioedema (C1 Esterase Inhibitor Deficiency) (human) (ingredient)
Complications:
This code is for airwayAirwayABCDE Assessment obstruction, the most life-threatening complication of angioedemaAngioedemaAngioedema is a localized, self-limited (but potentially life-threatening), nonpitting, asymmetrical edema occurring in the deep layers of the skin and mucosal tissue. The common underlying pathophysiology involves inflammatory mediators triggering significant vasodilation and increased capillary permeability. Angioedema, especially when it affects the larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy or tongueTongueThe tongue, on the other hand, is a complex muscular structure that permits tasting and facilitates the process of mastication and communication. The blood supply of the tongue originates from the external carotid artery, and the innervation is through cranial nerves.Lips and Tongue: Anatomy, which can lead to asphyxiation.
Coding System
Code
Description
ICD-10-CM
J38.4
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema of larynxLarynxThe larynx, also commonly called the voice box, is a cylindrical space located in the neck at the level of the C3-C6 vertebrae. The major structures forming the framework of the larynx are the thyroid cartilage, cricoid cartilage, and epiglottis. The larynx serves to produce sound (phonation), conducts air to the trachea, and prevents large molecules from reaching the lungs.Larynx: Anatomy
References
Frank Austen, K. (2008). Allergies, anaphylaxis, and systemic mastocytosis. In Fauci, A. S., Braunwald, E., Kasper, D. L., et al. (Eds.). Harrison’s Internal Medicine (17th ed., pp. 2065–2067).
Long B., Koyfman A., et al. (2019). Evaluation and management of angioedema in the emergency department. Western Journal of Emergency Medicine, 20(4), 587–600.
Moellman J., Bernstein J., et al.(2014). A consensus parameter for the evaluation and management of angioedema in the emergency department. Academic Emergency Medicine, 21(4), 469–484.
Bernstein, J. A., Cremonesi, P., Hoffmann, T. K., Hollingsworth, J. (2017). Angioedema in the emergency department: a practical guide to differential diagnosis and management. International Journal of Emergency Medicine, 10(1), 15. https://doi.org/10.1186/s12245-017-0141-z
Ferrante, G., Scavone, V., Muscia, M. C., Adrignola, E., Corsello, G., Passalacqua, G., La Grutta, S. (2015). The care pathway for children with urticaria, angioedema, mastocytosis. World Allergy Organization Journal, 8(1), 5. https://doi.org/10.1186/s40413-014-0052-x
Bowen, T., Cicardi, M., Farkas, H., Bork, K., Longhurst, H. J., Zuraw, B., Aygoeren-Pürsün, E., Craig, T., Binkley, K., Hebert, J., Ritchie, B., Bouillet, L., Betschel, S., Cogar, D., Dean, J., Devaraj, R., Hamed, A., Kamra, P., Keith, P. K., Lacuesta, G., … Xiang, Z. Y. (2010). 2010 International consensus algorithm for the diagnosis, therapy and management of hereditary angioedema. Allergy, Asthma & Clinical Immunology, 6(1), 24. https://doi.org/10.1186/1710-1492-6-24