Acute pancreatitis is an inflammatory disease of the pancreas due to autodigestion. Common etiologies include gallstones and excessive alcohol use. Patients typically present with epigastric pain radiating to the back. Diagnosis requires 2 of 3 criteria, including: characteristic abdominal pain, serum amylase and lipase 3 times the upper limit of normal, or characteristic radiology findings. Ranson criteria is commonly used to assess the severity. Management includes aggressive intravenous hydration, analgesia, nutritional support, and treatment of the underlying cause.
IncidenceIncidenceThe number of new cases of a given disease during a given period in a specified population. It also is used for the rate at which new events occur in a defined population. It is differentiated from prevalence, which refers to all cases in the population at a given time.Measures of Disease Frequency:
United States: 40–50 cases per 100,000 adults
Worldwide: 5–80 per 100,000 adults
Men > women
Men: likely due to alcohol
Women: related to biliary tractBiliary tractBile is secreted by hepatocytes into thin channels called canaliculi. These canaliculi lead into slightly larger interlobular bile ductules, which are part of the portal triads at the “corners” of hepatic lobules. The bile leaves the liver via the right and left hepatic ducts, which join together to form the common hepatic duct. Gallbladder and Biliary Tract: Anatomy disease
Necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis: 17%
Biliary tractBiliary tractBile is secreted by hepatocytes into thin channels called canaliculi. These canaliculi lead into slightly larger interlobular bile ductules, which are part of the portal triads at the “corners” of hepatic lobules. The bile leaves the liver via the right and left hepatic ducts, which join together to form the common hepatic duct. Gallbladder and Biliary Tract: Anatomy disease:
Approximately 40% of cases
Caused by biliary obstruction due to a stone
Alcohol use:
Approximately 30% of cases
Often an exacerbation of chronic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Usually seen with habitual consumption over 5–15 years, but may be seen after a binge
Endoscopic retrograde cholangiopancreatographyEndoscopic Retrograde CholangiopancreatographyFiberoptic endoscopy designed for duodenal observation and cannulation of Vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (Vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis (ERCPERCPFiberoptic endoscopy designed for duodenal observation and cannulation of vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis):
Can cause accidental lodging of stone into the sphincter of Oddi
AzathioprineAzathioprineAn immunosuppressive agent used in combination with cyclophosphamide and hydroxychloroquine in the treatment of rheumatoid arthritis. According to the fourth annual report on carcinogens, this substance has been listed as a known carcinogen.Immunosuppressants
Valproic acidValproic acidA fatty acid with anticonvulsant and anti-manic properties that is used in the treatment of epilepsy and bipolar disorder. The mechanisms of its therapeutic actions are not well understood. It may act by increasing gamma-aminobutyric acid levels in the brain or by altering the properties of voltage-gated sodium channels.First-Generation Anticonvulsant Drugs
Estrogens
ThiazideThiazideHeterocyclic compounds with sulfur and nitrogen in the ring. This term commonly refers to the benzothiadiazines that inhibit sodium-potassium-chloride symporters and are used as diuretics.Hyponatremia and loop diureticsDiureticsAgents that promote the excretion of urine through their effects on kidney function.Heart Failure and Chronic Coronary Syndrome Medication
OctreotideOctreotideA potent, long-acting synthetic somatostatin octapeptide analog that inhibits secretion of growth hormone and is used to treat hormone-secreting tumors; diabetes mellitus; hypotension, orthostatic; hyperinsulinism; hypergastrinemia; and small bowel fistula.Antidiarrheal Drugs
InfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease:
MumpsMumpsMumps is caused by a single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae. Mumps is typically a disease of childhood, which manifests initially with fever, muscle pain, headache, poor appetite, and a general feeling of malaise, and is classically followed by parotitis. Mumps Virus/Mumps
Hepatitis
CytomegalovirusCytomegalovirusCMV is a ubiquitous double-stranded DNA virus belonging to the Herpesviridae family. CMV infections can be transmitted in bodily fluids, such as blood, saliva, urine, semen, and breast milk. The initial infection is usually asymptomatic in the immunocompetent host, or it can present with symptoms of mononucleosis. Cytomegalovirus
CoxsackievirusCoxsackievirusCoxsackievirus is a member of a family of viruses called Picornaviridae and the genus Enterovirus. Coxsackieviruses are single-stranded, positive-sense RNA viruses, and are divided into coxsackie group A and B viruses. Both groups of viruses cause upper respiratory infections, rashes, aseptic meningitis, or encephalitis. Coxsackievirus
SalmonellaSalmonellaSalmonellae are gram-negative bacilli of the family Enterobacteriaceae. Salmonellae are flagellated, non-lactose-fermenting, and hydrogen sulfide-producing microbes. Salmonella enterica, the most common disease-causing species in humans, is further classified based on serotype as typhoidal (S. typhi and paratyphi) and nontyphoidal (S. enteritidis and typhimurium). Salmonella
Parasites
Genetic predispositions (e.g., CFTRmutationMutationGenetic mutations are errors in DNA that can cause protein misfolding and dysfunction. There are various types of mutations, including chromosomal, point, frameshift, and expansion mutations. Types of Mutations, as in cysticCysticFibrocystic ChangefibrosisFibrosisAny pathological condition where fibrous connective tissue invades any organ, usually as a consequence of inflammation or other injury.Bronchiolitis Obliterans)
HypercalcemiaHypercalcemiaHypercalcemia (serum calcium > 10.5 mg/dL) can result from various conditions, the majority of which are due to hyperparathyroidism and malignancy. Other causes include disorders leading to vitamin D elevation, granulomatous diseases, and the use of certain pharmacological agents. Symptoms vary depending on calcium levels and the onset of hypercalcemia. Hypercalcemia
Autoimmune pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis (IgG4)
Developmental:
Pancreatic ductus divisumPancreatic ductus divisumFailure of the dorsal and ventral pancreatic ducts to fuse.Acute Pancreatitis: failure of the dorsal and ventral pancreatic ducts to fuse
AnnularAnnularDermatologic ExaminationpancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy: a bandA bandSkeletal Muscle Contraction of pancreatic tissue surrounds the 2nd part of the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy
Acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis is classified according to the Revised Atlanta Classification system, which describes:
Severity:[15,16]
Mild:
Majority of cases
No local complications
No systemic complications/organ failure
Interstitial changesInterstitial changesPulmonary Function Tests in the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
Moderately severe:
Transient local complications, which may include fluid collections, pseudocysts, and areas of necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
Resolution of organ failure (typically involving respiratory, cardiovascular, and/or renal systems) in 48 hours
Interstitial edematous pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:
More common (approximately 80% of cases)
InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the pancreatic tissue causes interstitial edemaInterstitial EdemaIncreased Intracranial Pressure (ICP), which often resolves within 1 week.
Pancreatic blood supply is not disrupted.
Necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:
Pancreatic and/or peripancreatic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
Pancreatic blood supply interrupted.
Phases (can overlap):[15]
Early:
< 1 week since onset
Characterized by SIRS and/or organ failure
Organ failure and its duration determine the severity of the disease.
The course of the disease can be altered based on management done in this phase.
Phase in which pseudocysts and walled-off necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage develop
Acute peripancreatic fluid collection (APFC): inflammatory fluid without definable wall occuring in interstitial edematous pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis; typically resolve spontaneously
Acute necrotic collection (ANC): heterogeneous fluid without a wall associated with necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Collections > 4 weeks:
Pancreatic pseudocystPancreatic pseudocystCyst-like space not lined by epithelium and contained within the pancreas. Pancreatic pseudocysts account for most of the cystic collections in the pancreas and are often associated with chronic pancreatitis.Acute Cholangitis: encapsulatedEncapsulatedKlebsiella collection (with well-defined wall) typically developing from APFCs
Table: Acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis classification
Type
Interstitial edematous pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
CT findings
EdemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema is hypodense
Heterogeneous contrast enhancement
Necrotic areas show reduced contrast enhancement or lack thereof
Fluid collection ≤ 4 weeks (no definable wall)
Acute peripancreatic fluid collection
Acute necrotic collection
Fluid collection > 4 weeks (well-defined wall)
Pancreatic pseudocystPancreatic pseudocystCyst-like space not lined by epithelium and contained within the pancreas. Pancreatic pseudocysts account for most of the cystic collections in the pancreas and are often associated with chronic pancreatitis.Acute Cholangitis
Walled-off necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
Pathophysiology
Normal pancreatic function[7,14]
The pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy has endocrine (insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin) and exocrine (digestive enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes) functions.
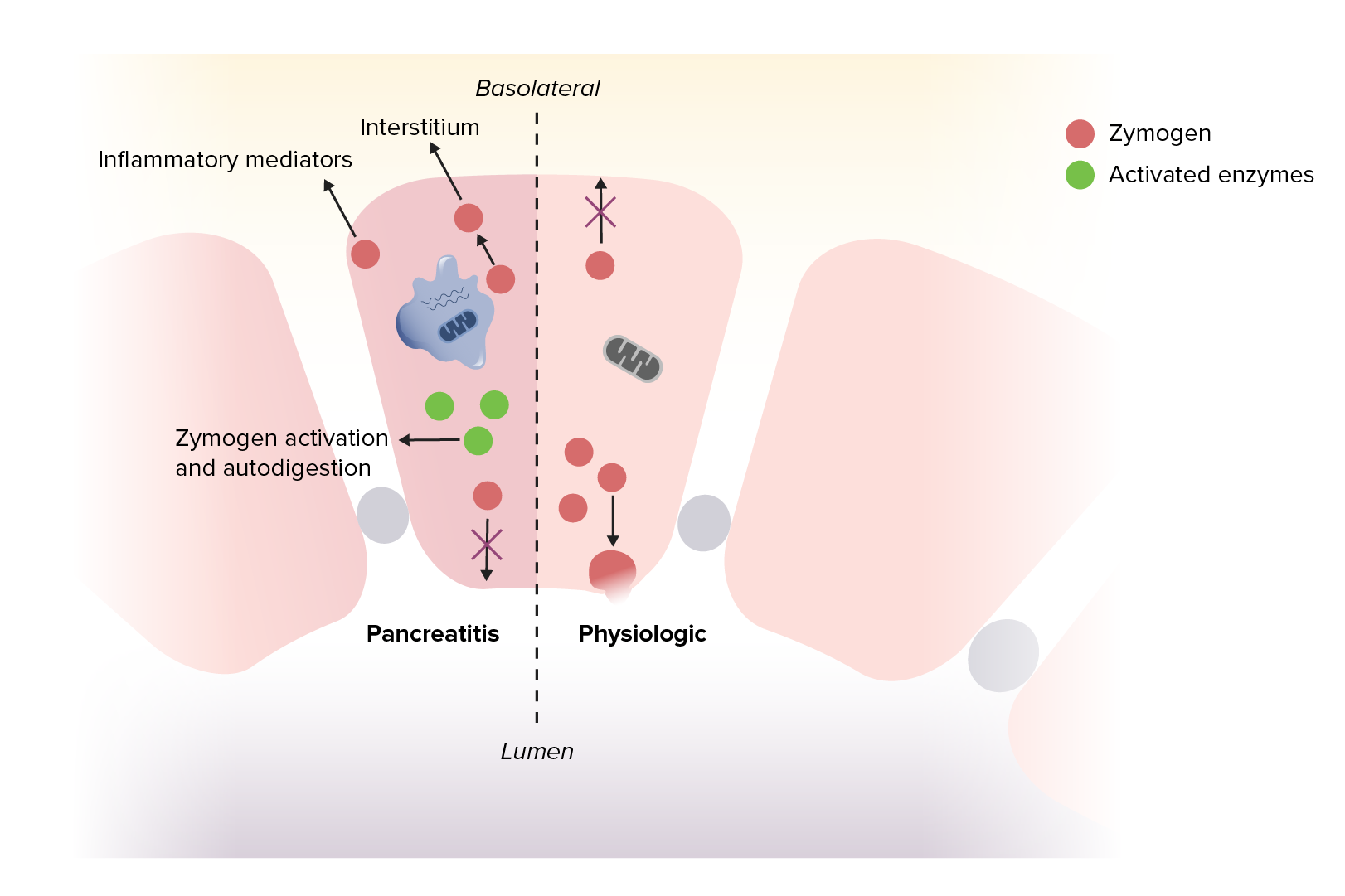
Digestive enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes made in acinar cellsAcinar cellsCells lining the saclike dilatations known as acini of various glands or the lungs.Gastrointestinal Secretions → stored as zymogens (inactive form) → released in the pancreatic duct and small intestineSmall intestineThe small intestine is the longest part of the GI tract, extending from the pyloric orifice of the stomach to the ileocecal junction. The small intestine is the major organ responsible for chemical digestion and absorption of nutrients. It is divided into 3 segments: the duodenum, the jejunum, and the ileum. Small Intestine: Anatomy → activation by trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides
Protective mechanisms against organ injury (autodigestion) include:
Negative feedbackNegative feedbackHypothalamic and Pituitary Hormones mechanism (↑ trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides in duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy → ↓ cholecystokininCholecystokininA peptide, of about 33 amino acids, secreted by the upper intestinal mucosa and also found in the central nervous system. It causes gallbladder contraction, release of pancreatic exocrine (or digestive) enzymes, and affects other gastrointestinal functions. Cholecystokinin may be the mediator of satiety.Gastrointestinal Secretions (CCK) and secretinSecretinA peptide hormone of about 27 amino acids from the duodenal mucosa that activates pancreatic secretion and lowers the blood sugar level.Gastrointestinal Secretions → ↓ pancreatic secretionSecretionCoagulation Studies)
Zymogens are controlled with protease inhibitorsProtease InhibitorsCompounds which inhibit or antagonize biosynthesis or actions of proteases (endopeptidases).Anti-HIV Drugs.
↓ Acinar cell pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance and calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes concentrations → prevent prematurePrematureChildbirth before 37 weeks of pregnancy (259 days from the first day of the mother’s last menstrual period, or 245 days after fertilization).Necrotizing Enterocolitis activation of trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides
Anything that disrupts the homeostasisHomeostasisThe processes whereby the internal environment of an organism tends to remain balanced and stable.Cell Injury and Death of normal pancreatic function can cause acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis pathogenesis[7,13,14,18]
Initiated through acinar cell injuryCell injuryThe cell undergoes a variety of changes in response to injury, which may or may not lead to cell death. Injurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Cell Injury and Death from:
Biliary obstruction → increased pancreatic duct pressure → acinar cell injuryCell injuryThe cell undergoes a variety of changes in response to injury, which may or may not lead to cell death. Injurious stimuli trigger the process of cellular adaptation, whereby cells respond to withstand the harmful changes in their environment. Overwhelmed adaptive mechanisms lead to cell injury. Mild stimuli produce reversible injury. If the stimulus is severe or persistent, injury becomes irreversible. Cell Injury and Death
Direct injury (e.g., toxins, alcohol)
Changes in acinar cell pHpHThe quantitative measurement of the acidity or basicity of a solution.Acid-Base Balance and calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes concentrations → allows intrapancreatic activation of trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides → activation of zymogens → autodigestion
Inhibited secretionSecretionCoagulation Studies on zymogens into the pancreatic ducts → exocytosisExocytosisCellular release of material within membrane-limited vesicles by fusion of the vesicles with the cell membrane.The Cell: Cell Membrane into the interstitium → not fully understood, but believed to lead to attraction of inflammatory cells
Inflammatory cells arrive → cytokine release → pancreatic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Cytokine release and vascular injury from enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes → vasodilationVasodilationThe physiological widening of blood vessels by relaxing the underlying vascular smooth muscle.Pulmonary Hypertension Drugs and vascular permeability → fluid shifting to the interstitial space (3rd spacing) → decreased perfusion and hypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension → can result in:
ShockShockShock is a life-threatening condition associated with impaired circulation that results in tissue hypoxia. The different types of shock are based on the underlying cause: distributive (↑ cardiac output (CO), ↓ systemic vascular resistance (SVR)), cardiogenic (↓ CO, ↑ SVR), hypovolemic (↓ CO, ↑ SVR), obstructive (↓ CO), and mixed. Types of Shock
Acute renal failureRenal failureConditions in which the kidneys perform below the normal level in the ability to remove wastes, concentrate urine, and maintain electrolyte balance; blood pressure; and calcium metabolism. Renal insufficiency can be classified by the degree of kidney damage (as measured by the level of proteinuria) and reduction in glomerular filtration rate.Crush Syndrome
Pancreatic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
Acute pancreatitis
Image by Lecturio.
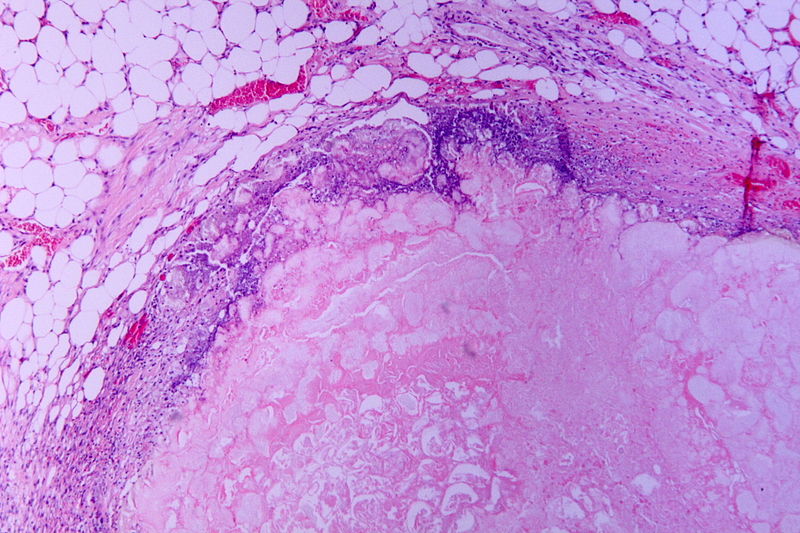
Hematoxylin and eosin (H&E) stain of necrotic pancreatitis (eosinophilic area without architecture: necrosis), surrounded by basophilic inflammatory cells and normal fat cells
Image: “Tryptic fat tissue necrosis in severe pancreatitis” by Patho. License: CC BY-SA 3.0.
RadiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma to the back (approximately 50% of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship)
NauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia
AnorexiaAnorexiaThe lack or loss of appetite accompanied by an aversion to food and the inability to eat. It is the defining characteristic of the disorder anorexia nervosa.Anorexia Nervosa
DiarrheaDiarrheaDiarrhea is defined as ≥ 3 watery or loose stools in a 24-hour period. There are a multitude of etiologies, which can be classified based on the underlying mechanism of disease. The duration of symptoms (acute or chronic) and characteristics of the stools (e.g., watery, bloody, steatorrheic, mucoid) can help guide further diagnostic evaluation. Diarrhea
TachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children
Diminished bowel sounds → ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction
Evidence of severe disease:
FeverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever
HypotensionHypotensionHypotension is defined as low blood pressure, specifically < 90/60 mm Hg, and is most commonly a physiologic response. Hypotension may be mild, serious, or life threatening, depending on the cause. Hypotension
Hepatomegaly → alcoholic pancreatitisAlcoholic pancreatitisAcute or chronic inflammation of the pancreas due to excessive alcohol drinking. Alcoholic pancreatitis usually presents as an acute episode but it is a chronic progressive disease in alcoholics.Chronic Pancreatitis
Scleral icterusScleral IcterusJaundice or jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice → choledocholithiasisCholedocholithiasisPresence or formation of gallstones in the common bile duct.Cholelithiasis
Muscle spasmsSpasmsAn involuntary contraction of a muscle or group of muscles. Spasms may involve skeletal muscle or smooth muscle.Ion Channel Myopathy → hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia
Warning signs of retroperitonealRetroperitonealPeritoneum: Anatomy bleeding in severe, necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:
Cullen’s signCullen’s signBluish discoloration around the umbilicus due to blood in the peritoneum.Acute Pancreatitis: bluish discoloration around the umbilicus due to blood in the peritoneumPeritoneumThe peritoneum is a serous membrane lining the abdominopelvic cavity. This lining is formed by connective tissue and originates from the mesoderm. The membrane lines both the abdominal walls (as parietal peritoneum) and all of the visceral organs (as visceral peritoneum).Peritoneum: Anatomy
Grey-Turner’s signGrey-Turner’s signReddish-brown discoloration on the flanks due to blood in the retroperitoneum or pancreatic exudates.Acute Pancreatitis: reddish-brown discoloration on the flanks due to blood in the retroperitoneum or pancreatic exudates
Cullen’s sign, signaling blood in the peritoneum
Image: “Cullen’s sign” by Herbert L. Fred, MD. License: CC BY 2.0.
Grey-Turner’s sign due to hemorrhagic pancreatitis
Image: by Herbert L. Fred, MD and Hendrik A. van Dijk. License: CC BY 2.0.
Diagnosis
Diagnostic criteria[3,19]
The diagnosis of acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis requires at least 2 of the following:
Serum amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption or lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion > 3 times the upper limitLimitA value (e.g., pressure or time) that should not be exceeded and which is specified by the operator to protect the lungInvasive Mechanical Ventilation of normal
Characteristic findings on imaging
Laboratory evaluation[1,15,18,19]
Pancreatic tests (enzymesEnzymesEnzymes are complex protein biocatalysts that accelerate chemical reactions without being consumed by them. Due to the body’s constant metabolic needs, the absence of enzymes would make life unsustainable, as reactions would occur too slowly without these molecules. Basics of Enzymes and other products):
↑ Serum amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption:
↑ within 6–12 hours of onset
Normalizes within 3–5 days in uncomplicated cases
Note: If presentation is > 24 hours after onset, amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption may be normal.
↑ Serum lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion (preferred test over amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption)
More specific for pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
↑ within 4–8 hours of onset, with peak onset at 24 hours
Normalizes within 8 days to 2 weeks
Urinary trypsinogenTrypsinogenThe inactive proenzyme of trypsin secreted by the pancreas, activated in the duodenum via cleavage by enteropeptidase.Pancreatic Parameters activation peptide (TAP):
Peptide cleaved from trypsinogenTrypsinogenThe inactive proenzyme of trypsin secreted by the pancreas, activated in the duodenum via cleavage by enteropeptidase.Pancreatic Parameters when trypsinTrypsinA serine endopeptidase that is formed from trypsinogen in the pancreas. It is converted into its active form by enteropeptidase in the small intestine. It catalyzes hydrolysis of the carboxyl group of either arginine or lysine.Proteins and Peptides is activated
Presence indicates early acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Metabolic tests:
Hepatic function tests
ALTALTAn enzyme that catalyzes the conversion of l-alanine and 2-oxoglutarate to pyruvate and l-glutamate.Liver Function Tests > 150 U/L and ↑ bilirubinBilirubinA bile pigment that is a degradation product of heme.Heme Metabolism → pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis secondary to gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis
CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes
↑ CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes → may be a potential cause of pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
↓ CalciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes → frequently seen, and should be corrected
Electrolyte imbalances can occur due to third spacing of fluids.
HyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus occurs owing to ↓ insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin release as well as ↑ glucagonGlucagonA 29-amino acid pancreatic peptide derived from proglucagon which is also the precursor of intestinal glucagon-like peptides. Glucagon is secreted by pancreatic alpha cells and plays an important role in regulation of blood glucose concentration, ketone metabolism, and several other biochemical and physiological processes.Gastrointestinal Secretions and catecholamine output.
↑ HematocritHematocritThe volume of packed red blood cells in a blood specimen. The volume is measured by centrifugation in a tube with graduated markings, or with automated blood cell counters. It is an indicator of erythrocyte status in disease. For example, anemia shows a low value; polycythemia, a high value.Neonatal Polycythemia → severe disease (due to hemoconcentrationHemoconcentrationNeonatal Polycythemia from third spacing of fluid)
↑ WBC → inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
C-reactive protein (CRP)
> 150 mg/L at 48 hours → risk of severe pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis and organ failure
ProcalcitoninProcalcitoninNeutropenic Fever: ↑ level predictive of progression to severe acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Hypertriglyceridemia-induced pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis (HTGP): Triglyceride levels have to be > 500 mg/dL (5.6 mmol/L) and are usually > 1000 mg/dL (11.3 mmol/L).
TriglyceridesTriglyceridesFatty Acids and Lipids > 1000 mg/dL: 5% risk of acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
TriglyceridesTriglyceridesFatty Acids and Lipids > 2000 mg/dL: up to 20% risk of acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Immunoglobulin G4 (IgG4)
May be checked if autoimmune pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis is suspected
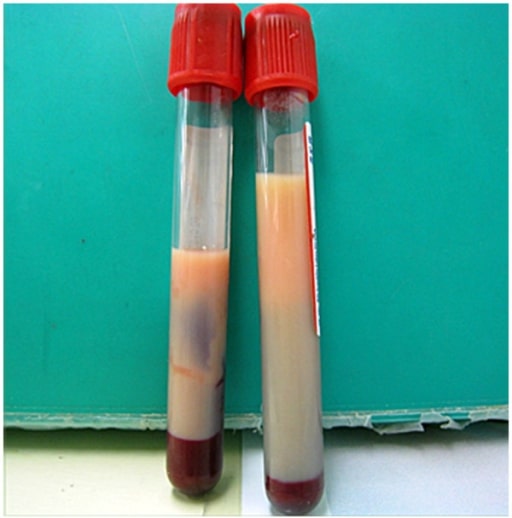
Milky plasma seen in a patient with hypertriglyceridemia: If seen, milky plasma should be considered as a potential cause of acute pancreatitis.
Image: “Milky plasma” by the Department of Emergency and Critical Care Medicine, Ohta Nishinouchi Hospital, 2-5-20 Nishinouchi, Koriyama, Fukushima, 963-8558, Japan. License: CC BY 2.0.
Imaging[2,9,15,16,18,19,21]
Imaging may not be required if the 1st 2 diagnostic criteria are metMETPreoperative Care, but can be used for evaluating the underlying cause and complications:
American College of Gastroenterologists (ACG) indications for imaging the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy with contrast-enhanced CT (or MRI):[15]
Diagnosis unclear
If individuals fail to improve after 48–72 hours
CT:
Normal in 30% of cases
Best performed 3–5 days after the onset of abdominal painAbdominal PainAcute Abdomen to determine presence of necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage or other complications
Potential findings:
Inflammatory changes of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
NecrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, fluid collections, or pseudocysts can be seen later in the course
Specific findings for interstitial edematous pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:
Diffusely or focally enlarged pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
Heterogeneous contrast enhancement
Mild inflammatory changes or peripancreatic stranding
Specific findings for necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:
Diffuse or focal necrotic areas
No (or decreased) pancreatic parenchymal enhancement in contrast studies
Peripancreatic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
Abdominal ultrasonography (US):
Can be done if gallstone pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis is suspected (recommended for all patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship by ACG)
Potential findings:
GallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis
Common bileBileAn emulsifying agent produced in the liver and secreted into the duodenum. Its composition includes bile acids and salts; cholesterol; and electrolytes. It aids digestion of fats in the duodenum.Gallbladder and Biliary Tract: Anatomy duct dilation
Pancreatic edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Peripancreatic fluid
Magnetic resonance cholangiopancreatogramMagnetic resonance cholangiopancreatogramNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Acute Pancreatitis (MRCPMRCPNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis)
Compared to CT with contrastCT with ContrastImaging of the Head and Brain, MRCPMRCPNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis has no radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma and gadoliniumGadoliniumAn element of the rare earth family of metals. It has the atomic symbol gd, atomic number 64, and atomic weight 157. 25. Its oxide is used in the control rods of some nuclear reactors.Magnetic Resonance Imaging (MRI) is less nephrotoxic.
Pancreatic edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema
Pancreatic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage or pseudocysts
Chest radiograph
For patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with pulmonary symptoms (dyspneaDyspneaDyspnea is the subjective sensation of breathing discomfort. Dyspnea is a normal manifestation of heavy physical or psychological exertion, but also may be caused by underlying conditions (both pulmonary and extrapulmonary). Dyspnea, tachypneaTachypneaIncreased respiratory rate.Pulmonary Examination, hypoxiaHypoxiaSub-optimal oxygen levels in the ambient air of living organisms.Ischemic Cell Damage)
Potential findings:
Pleural effusions
Basal atelectasisAtelectasisAtelectasis is the partial or complete collapse of a part of the lung. Atelectasis is almost always a secondary phenomenon from conditions causing bronchial obstruction, external compression, surfactant deficiency, or scarring. Atelectasis
Diffuse, patchy infiltrates indicating acute respiratory distress syndromeAcute Respiratory Distress SyndromeAcute respiratory distress syndrome is characterized by the sudden onset of hypoxemia and bilateral pulmonary edema without cardiac failure. Sepsis is the most common cause of ARDS. The underlying mechanism and histologic correlate is diffuse alveolar damage (DAD). Acute Respiratory Distress Syndrome (ARDS) (ARDS)
Abdominal radiograph
Limited role
“Sentinel loop” finding (short segment of ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction near the pancreatic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation)
ColonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy cutoff sign: abrupt termination of gas in the proximal colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy due to spasm of the descending colonDescending colonThe segment of large intestine between transverse colon and the sigmoid colon.Colon, Cecum, and Appendix: Anatomy
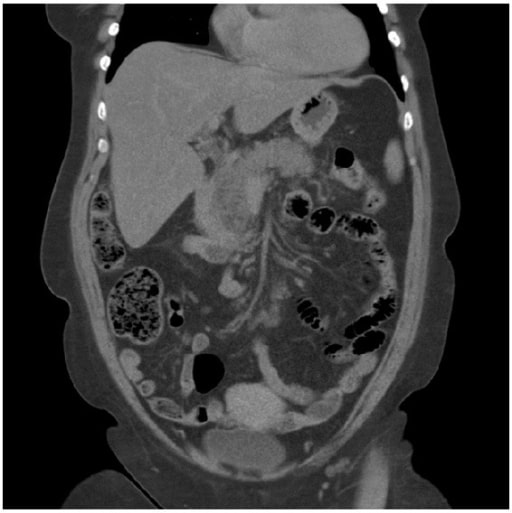
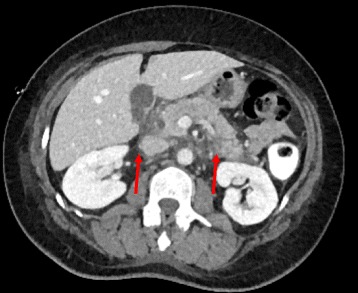
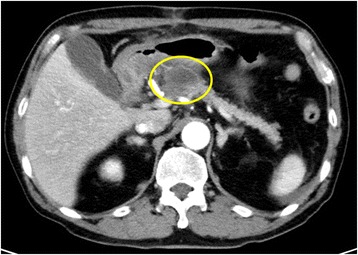
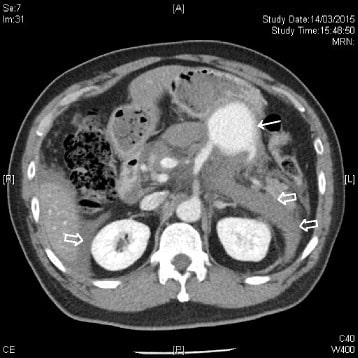
Acute pancreatitis: A CT scan showing pancreatitis changes, which appears enlarged and edematous.
Image: “A computed tomography scan” by Department of Surgery, Helsingborg Hospital, 25187 Helsingborg, Sweden. License: CC BY 3.0
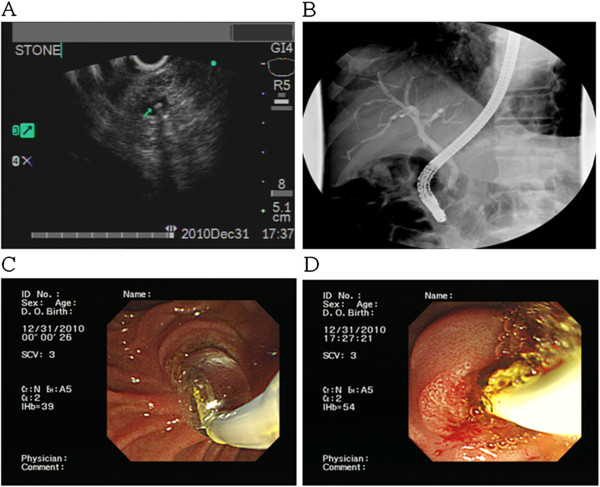
A tiny CBD stone is revealed using US. Such stones should be considered a potential etiology in a patient presenting with acute pancreatitis.
Image: “F2” by the Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, 386 Ta-Chung 1st Road, Kaohsiung 81362, Taiwan. License: CC BY 2.0, edited by Lecturio.
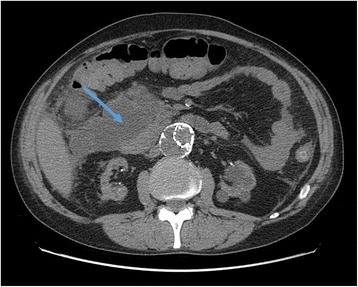
Acute pancreatitis on CT scan, showing edema around the pancreas
Image: “Arterial phase contrast CT showing an acute pancreatitis” by Benoît Bédat et al. License: CC BY 4.0.
PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas evaluation
Identifying the severity of acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis is helpful in order to ensure the patient is treated appropriately:
Ranson criteria:[1,16]
The biggest disadvantage is that it takes 48 hours to complete the assessment.
Evaluates age, temperature, mean arterial pressureMean Arterial PressureMean arterial pressure (MAP) is the average systemic arterial pressure and is directly related to cardiac output (CO) and systemic vascular resistance (SVR). The SVR and MAP are affected by the vascular anatomy as well as a number of local and neurohumoral factors.Vascular Resistance, Flow, and Mean Arterial Pressure, heart rateHeart rateThe number of times the heart ventricles contract per unit of time, usually per minute.Cardiac Physiology, respiratory rateRespiratory rateThe number of times an organism breathes with the lungs (respiration) per unit time, usually per minute.Pulmonary Examination, blood gas results, WBC count, electrolytesElectrolytesElectrolytes are mineral salts that dissolve in water and dissociate into charged particles called ions, which can be either be positively (cations) or negatively (anions) charged. Electrolytes are distributed in the extracellular and intracellular compartments in different concentrations. Electrolytes are essential for various basic life-sustaining functions.Electrolytes, creatinine, Glasgow ComaComaComa is defined as a deep state of unarousable unresponsiveness, characterized by a score of 3 points on the GCS. A comatose state can be caused by a multitude of conditions, making the precise epidemiology and prognosis of coma difficult to determine. ComaScaleScaleDermatologic Examination (GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma) score, and other health conditions
Severity is graded on the basis of the level of necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage, inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation, and findings of fluid collections.
Presence of necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage increases mortalityMortalityAll deaths reported in a given population.Measures of Health Status risk and affects the direction of treatment.
Modified CTSI:[9]
Incorporates extrapancreatic complications
Correlates better with outcome and organ failure
American College of Gastroenterology:[15]
Not a scoring system
In predicting severity, intrinsic patient factors are considered (e.g., age, body-mass index) along with other presenting findings (e.g., hypovolemiaHypovolemiaSepsis in Children, mental status); see table below.
Table: Ranson’s criteria (1 point each)
Present on admission
At 48 hours after admission
Age > 55 years
Decrease in hematocritHematocritThe volume of packed red blood cells in a blood specimen. The volume is measured by centrifugation in a tube with graduated markings, or with automated blood cell counters. It is an indicator of erythrocyte status in disease. For example, anemia shows a low value; polycythemia, a high value.Neonatal Polycythemia > 10%
WBC > 16,000/μL
Increase in BUN by ≥ 5 mg/dL
Blood glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance > 200 mg/dL
Serum CaCACondylomata acuminata are a clinical manifestation of genital HPV infection. Condylomata acuminata are described as raised, pearly, flesh-colored, papular, cauliflower-like lesions seen in the anogenital region that may cause itching, pain, or bleeding.Condylomata Acuminata (Genital Warts) < 8 mg/dL
AspartateAspartateOne of the non-essential amino acids commonly occurring in the l-form. It is found in animals and plants, especially in sugar cane and sugar beets. It may be a neurotransmitter.Synthesis of Nonessential Amino AcidstransaminaseTransaminaseA subclass of enzymes of the transferase class that catalyze the transfer of an amino group from a donor (generally an amino acid) to an acceptor (generally a 2-keto acid). Most of these enzymes are pyridoxyl phosphate proteins.Catabolism of Amino Acids (ASTASTEnzymes of the transferase class that catalyze the conversion of l-aspartate and 2-ketoglutarate to oxaloacetate and l-glutamate.Liver Function Tests) > 250 IU/L
Base deficit > 4 mEq/L
Estimated fluid sequestration > 6 L
0‒2: Minimal mortality
3‒5: 10%‒20% mortality rate, must be admitted to ICU
> 5: Increased risk of systemic complications and mortality
Definitions:
PaO2 is the partial pressure of oxygen in arterial blood.
GCSGCSA scale that assesses the response to stimuli in patients with craniocerebral injuries. The parameters are eye opening, motor response, and verbal response.Coma < 15
Pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion
Table: CT Severity Index (CTSI) and modified CTSI[9]
Characteristics
CTSI
MCTSI
Pancreatic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
Normal pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
0
0
Focal or diffuse enlargement of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
1
2
Intrinsic pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy abnormalities or peripancreatic inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation
2
2
Single acute fluid collection
3
4
≥ 2 acute fluid collections or peripancreatic gas
4
4
Pancreatic parenchymal necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage
None
0
0
< 30%
2
2
30–50%
4
4
> 50%
6
4
Extrapancreatic complications
Pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion, ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites, GI/vascular/parenchymal complications
N/A
2
Score interpretation
Maximum: 10
≥ 6 = severe disease
N/A: not applicable.
Table: American College of Gastroenterology: findings associated with a severe course (initial risk assessmentRisk assessmentThe qualitative or quantitative estimation of the likelihood of adverse effects that may result from exposure to specified health hazards or from the absence of beneficial influences.Preoperative Care)[15]
Patient risk factors
Age > 55 years
Body-mass index (BMIBMIAn indicator of body density as determined by the relationship of body weight to body height. Bmi=weight (kg)/height squared (m2). Bmi correlates with body fat (adipose tissue). Their relationship varies with age and gender. For adults, bmi falls into these categories: below 18. 5 (underweight); 18. 5-24. 9 (normal); 25. 0-29. 9 (overweight); 30. 0 and above (obese).Obesity) > 30
HematocritHematocritThe volume of packed red blood cells in a blood specimen. The volume is measured by centrifugation in a tube with graduated markings, or with automated blood cell counters. It is an indicator of erythrocyte status in disease. For example, anemia shows a low value; polycythemia, a high value.Neonatal Polycythemia > 44
Increasing hematocritHematocritThe volume of packed red blood cells in a blood specimen. The volume is measured by centrifugation in a tube with graduated markings, or with automated blood cell counters. It is an indicator of erythrocyte status in disease. For example, anemia shows a low value; polycythemia, a high value.Neonatal Polycythemia
Elevated creatinine
Radiologic findings
Pleural effusionPleural EffusionPleural effusion refers to the accumulation of fluid between the layers of the parietal and visceral pleura. Common causes of this condition include infection, malignancy, autoimmune disorders, or volume overload. Clinical manifestations include chest pain, cough, and dyspnea. Pleural Effusion
5–10 mL/kg/hr (ACG recommends 250–500 mL/hr) of isotonicIsotonicSolutions having the same osmotic pressure as blood serum, or another solution with which they are compared.Renal Sodium and Water RegulationcrystalloidCrystalloidIsotonic solutions of mineral salts, such as ringer’s lactate and sodium chloride (saline solution), used in fluid therapy to rehydrate blood volume.Intravenous Fluids solution (lactated Ringer [LR] solution or normal salineNormal salineA crystalloid solution that contains 9. 0g of sodium chloride per liter of water. It has a variety of uses, including: as a contact lens solution, in ophthalmic solutions and nasal lavage, in wound irrigation, and for fluid therapy.Intravenous Fluids)
Higher amount needed in those with severe volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration
LR is preferred if there are no contraindicationsContraindicationsA condition or factor associated with a recipient that makes the use of a drug, procedure, or physical agent improper or inadvisable. Contraindications may be absolute (life threatening) or relative (higher risk of complications in which benefits may outweigh risks).Noninvasive Ventilation.
In those with hypercalcemiaHypercalcemiaHypercalcemia (serum calcium > 10.5 mg/dL) can result from various conditions, the majority of which are due to hyperparathyroidism and malignancy. Other causes include disorders leading to vitamin D elevation, granulomatous diseases, and the use of certain pharmacological agents. Symptoms vary depending on calcium levels and the onset of hypercalcemia. Hypercalcemia, avoid LR (because of its calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes content).
Fluid intake and output monitoring
Goal urine output: 0.5 to 1 mL/kg/hr
Note that low urine output can be from volume depletionVolume depletionVolume status is a balance between water and solutes, the majority of which is Na. Volume depletion refers to a loss of both water and Na, whereas dehydration refers only to a loss of water. Volume depletion can be caused by GI losses, renal losses, bleeding, poor oral Na intake, or third spacing of fluids.Volume Depletion and Dehydration or acute tubular necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage.
Monitor BUN and hematocritHematocritThe volume of packed red blood cells in a blood specimen. The volume is measured by centrifugation in a tube with graduated markings, or with automated blood cell counters. It is an indicator of erythrocyte status in disease. For example, anemia shows a low value; polycythemia, a high value.Neonatal Polycythemia, as trends indicate severity.
Goal HR < 120 beats/min and a mean arterial pressureMean Arterial PressureMean arterial pressure (MAP) is the average systemic arterial pressure and is directly related to cardiac output (CO) and systemic vascular resistance (SVR). The SVR and MAP are affected by the vascular anatomy as well as a number of local and neurohumoral factors.Vascular Resistance, Flow, and Mean Arterial Pressure 65–85 mm Hg
Goal SpO₂ > 95%
Watch for signs of organ failure (especially cardiovascular and pulmonary).
With aggressive fluid administration, monitor for signs of pulmonary edemaPulmonary edemaPulmonary edema is a condition caused by excess fluid within the lung parenchyma and alveoli as a consequence of a disease process. Based on etiology, pulmonary edema is classified as cardiogenic or noncardiogenic. Patients may present with progressive dyspnea, orthopnea, cough, or respiratory failure.Pulmonary Edema.
Start oxygen support as indicated.
Address electrolyte imbalances
IV calcium gluconateCalcium gluconateThe calcium salt of gluconic acid. The compound has a variety of uses, including its use as a calcium replenisher in hypocalcemic states.Hypocalcemia for hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia (defined as a ↓ of serum corrected calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes of ≤ 7.5 mg/dL (calculator) or ionized calciumIonized CalciumHypocalcemia to ≤ 3 mg/dL)
IV magnesiumMagnesiumA metallic element that has the atomic symbol mg, atomic number 12, and atomic weight 24. 31. It is important for the activity of many enzymes, especially those involved in oxidative phosphorylation.Electrolytes for hypomagnesemiaHypomagnesemiaA nutritional condition produced by a deficiency of magnesium in the diet, characterized by anorexia, nausea, vomiting, lethargy, and weakness. Symptoms are paresthesias, muscle cramps, irritability, decreased attention span, and mental confusion, possibly requiring months to appear. Deficiency of body magnesium can exist even when serum values are normal. In addition, magnesium deficiency may be organ-selective, since certain tissues become deficient before others. Electrolytes (which leads to ↓ calciumCalciumA basic element found in nearly all tissues. It is a member of the alkaline earth family of metals with the atomic symbol ca, atomic number 20, and atomic weight 40. Calcium is the most abundant mineral in the body and combines with phosphorus to form calcium phosphate in the bones and teeth. It is essential for the normal functioning of nerves and muscles and plays a role in blood coagulation (as factor IV) and in many enzymatic processes.Electrolytes)
InsulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin therapy for hyperglycemiaHyperglycemiaAbnormally high blood glucose level.Diabetes Mellitus
Medications:
Analgesics (typically opioidsOpioidsOpiates are drugs that are derived from the sap of the opium poppy. Opiates have been used since antiquity for the relief of acute severe pain. Opioids are synthetic opiates with properties that are substantially similar to those of opiates. Opioid Analgesics), usually administered via patient-controlled analgesiaAnalgesiaMethods of pain relief that may be used with or in place of analgesics.Anesthesiology: History and Basic Concepts (IV fentanylFentanylA potent narcotic analgesic, abuse of which leads to habituation or addiction. It is primarily a mu-opioid agonist. Fentanyl is also used as an adjunct to general anesthetics, and as an anesthetic for induction and maintenance.Opioid Analgesics or hydromorphoneHydromorphoneAn opioid analgesic made from morphine and used mainly as an analgesic. It has a shorter duration of action than morphine.Opioid Analgesics)
AntiemeticsAntiemeticsAntiemetics are medications used to treat and/or prevent nausea and vomiting. These drugs act on different target receptors. The main classes include benzodiazepines, corticosteroids, atypical antipsychotics, cannabinoids, and antagonists of the following receptors: serotonin, dopamine, and muscarinic and neurokinin receptors.Antiemetics
Initial bowel rest
Early nutritional support:
Can be started as early as 24 hours, if painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways is decreasing
Is associated with ↓ morbidityMorbidityThe proportion of patients with a particular disease during a given year per given unit of population.Measures of Health Status compared to delayed or no nutrition
Rule out ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction before initiating
Setting and specific nutrition:[3,15,17–20,22]
Mild acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:
Can be treated on a general medical ward
May begin low-residue, low-fat diet as soon as tolerated
Severe acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis:
Intensive care setting preferred
May require enteral nutritionEnteral nutritionNutritional support given via the alimentary canal or any route connected to the gastrointestinal system (i.e., the enteral route). This includes oral feeding, sip feeding, and tube feeding using nasogastric, gastrostomy, and jejunostomy tubes.Short Bowel Syndrome if the patient cannot tolerate oral intake
Start within 72 hours
Enteral nutritionEnteral nutritionNutritional support given via the alimentary canal or any route connected to the gastrointestinal system (i.e., the enteral route). This includes oral feeding, sip feeding, and tube feeding using nasogastric, gastrostomy, and jejunostomy tubes.Short Bowel Syndrome maintains gut barrier function and prevents bacterial translocation.
Either nasogastric or naso-enteral route
Use high-protein, low-fat, semi-elemental feeding formulas.
Parenteral nutritionParenteral nutritionThe administering of nutrients for assimilation and utilization by a patient who cannot maintain adequate nutrition by enteral feeding alone. Nutrients are administered by a route other than the alimentary canal (e.g., intravenously, subcutaneously).Central Venous Catheter is given if enteral feeding is not tolerated or not advancing.
Antibiotics:[15,18.19]
Prophylactic antibiotics are not recommended.
Extrapancreatic infectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease (e.g., urinary tractUrinary tractThe urinary tract is located in the abdomen and pelvis and consists of the kidneys, ureters, urinary bladder, and urethra. The structures permit the excretion of urine from the body. Urine flows from the kidneys through the ureters to the urinary bladder and out through the urethra.Urinary Tract: AnatomyinfectionsInfectionsInvasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases.Chronic Granulomatous Disease, pneumoniaPneumoniaPneumonia or pulmonary inflammation is an acute or chronic inflammation of lung tissue. Causes include infection with bacteria, viruses, or fungi. In more rare cases, pneumonia can also be caused through toxic triggers through inhalation of toxic substances, immunological processes, or in the course of radiotherapy.Pneumonia) are treated with the appropriate antibiotics.
Consider giving antibiotics for infected necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage:
In those with necrotic pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis who do not improve in 7 days
Empiric options: carbapenemsCarbapenemsA group of beta-lactam antibiotics in which the sulfur atom in the thiazolidine ring of the penicillin molecule is replaced by a carbon atom. Thienamycins are a subgroup of carbapenems which have a sulfur atom as the first constituent of the side chain.Carbapenems and Aztreonam, quinolonesQuinolonesA group of derivatives of naphthyridine carboxylic acid, quinoline carboxylic acid, or nalidixic acid.Fluoroquinolones, and metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess
Treating the etiology
GallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis:[3,15,18,19]
CholedocholithiasisCholedocholithiasisPresence or formation of gallstones in the common bile duct.Cholelithiasis can result in pancreatic duct and/or biliary treeBiliary treeThe bile ducts and the gallbladder.Gallbladder and Biliary Tract: Anatomy obstruction, leading to severe acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Persistent elevation of liver function testsLiver function testsLiver function tests, also known as hepatic function panels, are one of the most commonly performed screening blood tests. Such tests are also used to detect, evaluate, and monitor acute and chronic liver diseases.Liver Function Tests → suspect obstruction
Endoscopic US or MRCPMRCPNon-invasive diagnostic technique for visualizing the pancreatic ducts and bile ducts without the use of injected contrast media or x-ray. Mri scans provide excellent sensitivity for duct dilatation, biliary stricture, and intraductal abnormalities.Primary Sclerosing Cholangitis helps determine the presence of obstruction.
Endoscopic retrograde cholangiopancreatographyEndoscopic Retrograde CholangiopancreatographyFiberoptic endoscopy designed for duodenal observation and cannulation of Vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (Vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis (ERCPERCPFiberoptic endoscopy designed for duodenal observation and cannulation of vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis):
Can perform sphincterotomySphincterotomySurgical incision of a sphincter.Anal Fissure and stone extraction
Indicated for choledocholithiasisCholedocholithiasisPresence or formation of gallstones in the common bile duct.Cholelithiasis or evidence of cholangitis
Note: Acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis is the most common complication of ERCPERCPFiberoptic endoscopy designed for duodenal observation and cannulation of vater’s ampulla, in order to visualize the pancreatic and biliary duct system by retrograde injection of contrast media. Endoscopic (vater) papillotomy may be performed during this procedure.Primary Sclerosing Cholangitis.[3]
CholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy
Surgical removal of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy
Performed after recovery from pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Without surgery, there is an increased risk of recurrent pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, cholangitis or cholecystitisCholecystitisCholecystitis is the inflammation of the gallbladder (GB) usually caused by the obstruction of the cystic duct (acute cholecystitis). Mechanical irritation by gallstones can also produce chronic GB inflammation. Cholecystitis is one of the most common complications of cholelithiasis but inflammation without gallstones can occur in a minority of patients. Cholecystitis.[15]
IV insulinInsulinInsulin is a peptide hormone that is produced by the beta cells of the pancreas. Insulin plays a role in metabolic functions such as glucose uptake, glycolysis, glycogenesis, lipogenesis, and protein synthesis. Exogenous insulin may be needed for individuals with diabetes mellitus, in whom there is a deficiency in endogenous insulin or increased insulin resistance. Insulin
Activates lipoprotein lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion (LPL), resulting in the removal of triglyceridesTriglyceridesFatty Acids and Lipids from the plasmaPlasmaThe residual portion of blood that is left after removal of blood cells by centrifugation without prior blood coagulation.Transfusion Products
Requires close glucoseGlucoseA primary source of energy for living organisms. It is naturally occurring and is found in fruits and other parts of plants in its free state. It is used therapeutically in fluid and nutrient replacement.Lactose Intolerance monitoring
May need a concurrent dextroseDextroseIntravenous Fluids infusion to prevent hypoglycemiaHypoglycemiaHypoglycemia is an emergency condition defined as a serum glucose level ≤ 70 mg/dL (≤ 3.9 mmol/L) in diabetic patients. In nondiabetic patients, there is no specific or defined limit for normal serum glucose levels, and hypoglycemia is defined mainly by its clinical features. Hypoglycemia
Apheresis
Rapidly decreases triglyceride levels
Should be considered in patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with SIRS, hypocalcemiaHypocalcemiaHypocalcemia, a serum calcium < 8.5 mg/dL, can result from various conditions. The causes may include hypoparathyroidism, drugs, disorders leading to vitamin D deficiency, and more. Calcium levels are regulated and affected by different elements such as dietary intake, parathyroid hormone (PTH), vitamin D, pH, and albumin. Presentation can range from an asymptomatic (mild deficiency) to a life-threatening condition (acute, significant deficiency). Hypocalcemia, and multi-organ dysfunctionMulti-Organ DysfunctionToxic Shock Syndrome
Infected pancreatic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage or abscessAbscessAccumulation of purulent material in tissues, organs, or circumscribed spaces, usually associated with signs of infection.Chronic Granulomatous Disease[15–19]
Walled-off necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage:
Develops as an encapsulatedEncapsulatedKlebsiella pancreatic or peripancreatic collection at least 4 weeks after acute necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Bacterial translocation from the colonColonThe large intestines constitute the last portion of the digestive system. The large intestine consists of the cecum, appendix, colon (with ascending, transverse, descending, and sigmoid segments), rectum, and anal canal. The primary function of the colon is to remove water and compact the stool prior to expulsion from the body via the rectum and anal canal. Colon, Cecum, and Appendix: Anatomy
SeedingSeedingThe local implantation of tumor cells by contamination of instruments and surgical equipment during and after surgical resection, resulting in local growth of the cells and tumor formation.Grading, Staging, and Metastasis from bacteremiaBacteremiaThe presence of viable bacteria circulating in the blood. Fever, chills, tachycardia, and tachypnea are common acute manifestations of bacteremia. The majority of cases are seen in already hospitalized patients, most of whom have underlying diseases or procedures which render their bloodstreams susceptible to invasion.Glycopeptides (which can occur during intubationIntubationPeritonsillar Abscess or IV lineIv LineCentral Venous Catheter placement)
CT or MRI findings:
Heterogeneous fluid collection consisting of liquid and non-liquid components, with loculation
A well-defined wall encapsulates the fluid collection.
Can be intrapancreatic and/or extrapancreatic
No internal septa within the cyst cavity
Consider if patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship continue to have a feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever or increasing leukocytosisLeukocytosisA transient increase in the number of leukocytes in a body fluid.West Nile Virus
One-third of patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship with pancreatic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage will develop infection.
Causative organisms:
E. coli
PseudomonasPseudomonasPseudomonas is a non-lactose-fermenting, gram-negative bacillus that produces pyocyanin, which gives it a characteristic blue-green color. Pseudomonas is found ubiquitously in the environment, as well as in moist reservoirs, such as hospital sinks and respiratory equipment. Pseudomonas
KlebsiellaKlebsiellaKlebsiella are encapsulated gram-negative, lactose-fermenting bacilli. They form pink colonies on MacConkey agar due to lactose fermentation. The main virulence factor is a polysaccharide capsule. Klebsiella pneumoniae is the most important pathogenic species.Klebsiella
EnterococcusEnterococcusEnterococcus is a genus of oval-shaped gram-positive cocci that are arranged in pairs or short chains. Distinguishing factors include optochin resistance and the presence of pyrrolidonyl arylamidase (PYR) and Lancefield D antigen. Enterococcus is part of the normal flora of the human GI tract.Enterococcus
Treatment:[16]
Antibiotics: given preoperatively (prior to drainage) and continued with choices dictated by culture and sensitivity results:
CarbapenemsCarbapenemsA group of beta-lactam antibiotics in which the sulfur atom in the thiazolidine ring of the penicillin molecule is replaced by a carbon atom. Thienamycins are a subgroup of carbapenems which have a sulfur atom as the first constituent of the side chain.Carbapenems and Aztreonam (initial antibiotic of choice)
FluoroquinolonesFluoroquinolonesFluoroquinolones are a group of broad-spectrum, bactericidal antibiotics inhibiting bacterial DNA replication. Fluoroquinolones cover gram-negative, anaerobic, and atypical organisms, as well as some gram-positive and multidrug-resistant (MDR) organisms. Fluoroquinolones with metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess
CefepimeCefepimeA fourth-generation cephalosporin antibacterial agent that is used in the treatment of infections, including those of the abdomen, urinary tract, respiratory tract, and skin. It is effective against pseudomonas aeruginosa and may also be used in the empiric treatment of febrile neutropenia.Cephalosporins or ceftazidimeCeftazidimeSemisynthetic, broad-spectrum antibacterial derived from cephaloridine and used especially for pseudomonas and other gram-negative infections in debilitated patients.Cephalosporins with metronidazoleMetronidazoleA nitroimidazole used to treat amebiasis; vaginitis; trichomonas infections; giardiasis; anaerobic bacteria; and treponemal infections.Pyogenic Liver Abscess
Image-guided aspiration and drainage:
Percutaneous CT-guided catheter drainage allows decompression and removal of necrotic debris with irrigation.
Uses local anesthesiaAnesthesiaA state characterized by loss of feeling or sensation. This depression of nerve function is usually the result of pharmacologic action and is induced to allow performance of surgery or other painful procedures.Anesthesiology: History and Basic Concepts, permitting drainage for those who are unable to undergo major surgery
A pancreaticocutaneous fistulaFistulaAbnormal communication most commonly seen between two internal organs, or between an internal organ and the surface of the body.Anal Fistula can develop.
Endoscopic debridementDebridementThe removal of foreign material and devitalized or contaminated tissue from or adjacent to a traumatic or infected lesion until surrounding healthy tissue is exposed.Stevens-Johnson Syndrome:
Indicated in individuals who fail to improve with antibiotics (often given for > 4 weeks)
Performed under conscious sedation
Fluid collection is identified via endoscopic US
Cystenterostomy is created, and debridementDebridementThe removal of foreign material and devitalized or contaminated tissue from or adjacent to a traumatic or infected lesion until surrounding healthy tissue is exposed.Stevens-Johnson Syndrome is performed.
A nasocystic tube allows further lavage.
Surgical necrosectomy (debridementDebridementThe removal of foreign material and devitalized or contaminated tissue from or adjacent to a traumatic or infected lesion until surrounding healthy tissue is exposed.Stevens-Johnson Syndrome of pancreatic necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage) if less invasive measures are not successful
Abdominal CT scan showing the initial area of patchy necrosis around the head of the pancreas
Image: “Abdominal CT scan” by Francesco Fontana. License: CC BY 4.0.
CT scans in a patient who developed infected pancreatic necrosis: A: Extensive pancreatic necrosis with a large amount of gas is seen in the body and tail of the pancreas. B: After 60 days of follow-up, a small decrease in the collection of gas is noted. C: 4 months after hospital discharge: atrophy of pancreatic parenchyma
Image: “CT scan” by Roberto Rasslan et al. License: CC BY 4.0
Pseudocyst[8,16,17]
An encapsulatedEncapsulatedKlebsiella collection of fluid with a well-defined inflammatory wall
Occurs several weeks after the onset of pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis (interstitial edematous type)
Most are asymptomatic, but some may have abdominal painAbdominal PainAcute Abdomen, early satietyEarly SatietyBariatric Surgery, or jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice
Diagnosis is made with US, CT, or MRI, with findings as follows:[16]
Follow-up imaging (CT or MRI) obtained in 3–6 months, with no further intervention done for those showing resolution or decrease in size
Obtain imaging earlier if symptoms (abdominal painAbdominal PainAcute Abdomen, feverFeverFever is defined as a measured body temperature of at least 38°C (100.4°F). Fever is caused by circulating endogenous and/or exogenous pyrogens that increase levels of prostaglandin E2 in the hypothalamus. Fever is commonly associated with chills, rigors, sweating, and flushing of the skin. Fever, vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia, jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice) develop.
Drainage:
For those who are symptomatic or develop infection
Requires the wall of the pseudocyst to mature, which may take weeks
Most collections are adherent to the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy or duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy, allowing endoscopic ultrasonography (EUS)-guided transmural drainage.
Surgical drainage is done if endoscopic drainage is unsuccessful.
Acute pancreatitis repeatedly occurred 1 month after the 1st operation, and a pancreatic pseudocyst developed at the same site. Enhanced CT showed a cyst with a diameter of 29 mm in the body of the pancreas.
Image: “Pancreatic pseudocyst” by the Department of Gastroenterological Surgery, Kumamoto University Graduate School of Medical Sciences, 1-1-1 Honjo, Kumamoto, 860-8556 Japan. License: CC BY 4.0.
Sustained intra-abdominal pressure (IAP) with organ failure
Due to significant tissue edemaEdemaEdema is a condition in which excess serous fluid accumulates in the body cavity or interstitial space of connective tissues. Edema is a symptom observed in several medical conditions. It can be categorized into 2 types, namely, peripheral (in the extremities) and internal (in an organ or body cavity). Edema, ascitesAscitesAscites is the pathologic accumulation of fluid within the peritoneal cavity that occurs due to an osmotic and/or hydrostatic pressure imbalance secondary to portal hypertension (cirrhosis, heart failure) or non-portal hypertension (hypoalbuminemia, malignancy, infection).Ascites, ileusIleusA condition caused by the lack of intestinal peristalsis or intestinal motility without any mechanical obstruction. This interference of the flow of intestinal contents often leads to intestinal obstruction. Ileus may be classified into postoperative, inflammatory, metabolic, neurogenic, and drug-induced.Small Bowel Obstruction, and/or fluid resuscitationResuscitationThe restoration to life or consciousness of one apparently dead. .Neonatal Respiratory Distress Syndrome[12]
↑ IAP:[6]
For most individuals, normal intra-abdominal pressure is 5–7 mm Hg.
Compartment syndromeCompartment SyndromeCompartment syndrome is a surgical emergency usually occurring secondary to trauma. The condition is marked by increased pressure within a compartment that compromises the circulation and function of the tissues within that space.Compartment Syndrome: extended IAP > 20 mm Hg with new-onset organ failure
Diaphragmatic elevation and subsequent compressionCompressionBlunt Chest Trauma of the lung, causing atelectasisAtelectasisAtelectasis is the partial or complete collapse of a part of the lung. Atelectasis is almost always a secondary phenomenon from conditions causing bronchial obstruction, external compression, surfactant deficiency, or scarring. Atelectasis and reduced oxygen diffusionDiffusionThe tendency of a gas or solute to pass from a point of higher pressure or concentration to a point of lower pressure or concentration and to distribute itself throughout the available space. Diffusion, especially facilitated diffusion, is a major mechanism of biological transport.Peritoneal Dialysis and Hemodialysis
Progressive oliguriaOliguriaDecreased urine output that is below the normal range. Oliguria can be defined as urine output of less than or equal to 0. 5 or 1 ml/kg/hr depending on the age.Renal Potassium Regulation
Hemodynamic instability
Pulmonary decompensation
Diagnosis is made by measuring the intra-abdominal pressure (intravesical pressure).
Treatment:
Hemodynamic support
PainPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways control
Surgical decompression (for individuals with IAPs > 25 mm Hg):
PseudoaneurysmPseudoaneurysmNot an aneurysm but a well-defined collection of blood and connective tissue outside the wall of a blood vessel or the heart. It is the containment of a ruptured blood vessel or heart, such as sealing a rupture of the left ventricle. False aneurysm is formed by organized thrombus and hematoma in surrounding tissue.Thoracic Aortic Aneurysms[12]
Results from the erosionErosionPartial-thickness loss of the epidermisGeneralized and Localized Rashes of the gastroduodenal or splenic artery (most commonly affected) into a pseudocyst
Rare, but life-threatening
Presents with unexplained GI bleeding and anemiaAnemiaAnemia is a condition in which individuals have low Hb levels, which can arise from various causes. Anemia is accompanied by a reduced number of RBCs and may manifest with fatigue, shortness of breath, pallor, and weakness. Subtypes are classified by the size of RBCs, chronicity, and etiology. Anemia: Overview and Types:[4]
Increased bleeding into the cyst can lead to rupture.
Blood may go to the peritoneal cavityPeritoneal CavityThe space enclosed by the peritoneum. It is divided into two portions, the greater sac and the lesser sac or omental bursa, which lies behind the stomach. The two sacs are connected by the foramen of winslow, or epiploic foramen.Peritoneum: Anatomy.
Blood may travel via the pancreatic duct into the duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy (hemosuccus pancreaticus).
AngiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery for diagnosis and embolizationEmbolizationA method of hemostasis utilizing various agents such as gelfoam, silastic, metal, glass, or plastic pellets, autologous clot, fat, and muscle as emboli. It has been used in the treatment of spinal cord and intracranial arteriovenous malformations, renal arteriovenous fistulas, gastrointestinal bleeding, epistaxis, hypersplenism, certain highly vascular tumors, traumatic rupture of blood vessels, and control of operative hemorrhage.Gastrointestinal Bleeding
CT scan of the abdomen with IV contrast showing a contrast-enhanced mass (solid arrow) at the splenic artery (branching from the superior mesenteric artery) compatible with a splenic artery pseudoaneurysm. Hemoretroperitoneum and hemoperitoneum were demonstrated (hollow arrows).
Image: “CT scan of the abdomen” by the Accident and Emergency Department, Ruttonjee Hospital, Wanchai, Hong Kong. License: CC BY 4.0.
Contrast-enhanced CT scan of the abdomen reveals a 5 × 6 × 7 cm complex cystic mass in the region of the uncinate process of the pancreatic head with an enhancing capsule and a small hyperdensity consistent with pseudoaneurysm of a peripancreatic vessel with active bleeding into the pancreatic pseudocyst.
Image: “Contrast-enhanced CT scan” by Rohan Mandaliya. License: CC BY 2.0.
ThrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus of the splenic, portal, or superior mesenteric veinsVeinsVeins are tubular collections of cells, which transport deoxygenated blood and waste from the capillary beds back to the heart. Veins are classified into 3 types: small veins/venules, medium veins, and large veins. Each type contains 3 primary layers: tunica intima, tunica media, and tunica adventitia. Veins: Histology
This is, many times, found incidentally on imaging
Treatment
Treat the underlying pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
AnticoagulationAnticoagulationPulmonary Hypertension Drugs if compromising hepatic function (portal veinPortal veinA short thick vein formed by union of the superior mesenteric vein and the splenic vein.Liver: AnatomythrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus) or bowel perfusion (superior mesenteric vein thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus)
ARDS[12,14]
Respiratory failureRespiratory failureRespiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure with widespread alveolar damage and inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the lungsLungsLungs are the main organs of the respiratory system. Lungs are paired viscera located in the thoracic cavity and are composed of spongy tissue. The primary function of the lungs is to oxygenate blood and eliminate CO2. Lungs: Anatomy
Mediated by cytokinesCytokinesNon-antibody proteins secreted by inflammatory leukocytes and some non-leukocytic cells, that act as intercellular mediators. They differ from classical hormones in that they are produced by a number of tissue or cell types rather than by specialized glands. They generally act locally in a paracrine or autocrine rather than endocrine manner.Adaptive Immune Response and inflammatory cells
Caused by systemic inflammationSystemic InflammationSurgical Site Infections from acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis
Chest radiograph will show diffuse, bilateral opacities
Treatment
Oxygen supplementation
High flowFlowBlood flows through the heart, arteries, capillaries, and veins in a closed, continuous circuit. Flow is the movement of volume per unit of time. Flow is affected by the pressure gradient and the resistance fluid encounters between 2 points. Vascular resistance is the opposition to flow, which is caused primarily by blood friction against vessel walls.Vascular Resistance, Flow, and Mean Arterial Pressurenasal cannulaNasal CannulaRespiratory Failure
Acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis: inflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy resulting from sustained gallstone impaction of the cysticCysticFibrocystic Change duct. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with colicky, upper abdominal painAbdominal PainAcute Abdomen, nauseaNauseaAn unpleasant sensation in the stomach usually accompanied by the urge to vomit. Common causes are early pregnancy, sea and motion sickness, emotional stress, intense pain, food poisoning, and various enteroviruses.Antiemetics, and vomitingVomitingThe forcible expulsion of the contents of the stomach through the mouth.Hypokalemia. InflammationInflammationInflammation is a complex set of responses to infection and injury involving leukocytes as the principal cellular mediators in the body’s defense against pathogenic organisms. Inflammation is also seen as a response to tissue injury in the process of wound healing. The 5 cardinal signs of inflammation are pain, heat, redness, swelling, and loss of function. Inflammation of the gallbladderGallbladderThe gallbladder is a pear-shaped sac, located directly beneath the liver, that sits on top of the superior part of the duodenum. The primary functions of the gallbladder include concentrating and storing up to 50 mL of bile. Gallbladder and Biliary Tract: Anatomy and gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis are seen on US or CT. AmylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption and lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion are usually not elevated, which differentiates acute cholecystitisAcute cholecystitisAcute inflammation of the gallbladder wall. It is characterized by the presence of abdominal pain; fever; and leukocytosis. Gallstone obstruction of the cystic duct is present in approximately 90% of the cases.Cholecystitis from acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis. Treatment includes IVF, antibiotics, and cholecystectomyCholecystectomyCholecystectomy is a surgical procedure performed with the goal of resecting and extracting the gallbladder. It is one of the most common abdominal surgeries performed in the Western world. Cholecystectomy is performed for symptomatic cholelithiasis, cholecystitis, gallbladder polyps > 0.5 cm, porcelain gallbladder, choledocholithiasis and gallstone pancreatitis, and rarely, for gallbladder cancer. Cholecystectomy.
Perforated peptic ulcerPeptic ulcerPeptic ulcer disease (PUD) refers to the full-thickness ulcerations of duodenal or gastric mucosa. The ulcerations form when exposure to acid and digestive enzymes overcomes mucosal defense mechanisms. The most common etiologies include Helicobacter pylori (H. pylori) infection and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). Peptic Ulcer Disease disease: complete erosionErosionPartial-thickness loss of the epidermisGeneralized and Localized Rashes of an ulcer through the wall of the stomachStomachThe stomach is a muscular sac in the upper left portion of the abdomen that plays a critical role in digestion. The stomach develops from the foregut and connects the esophagus with the duodenum. Structurally, the stomach is C-shaped and forms a greater and lesser curvature and is divided grossly into regions: the cardia, fundus, body, and pylorus. Stomach: Anatomy or duodenumDuodenumThe shortest and widest portion of the small intestine adjacent to the pylorus of the stomach. It is named for having the length equal to about the width of 12 fingers.Small Intestine: Anatomy. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship present with severe epigastric painEpigastric painMallory-Weiss Syndrome (Mallory-Weiss Tear), tachycardiaTachycardiaAbnormally rapid heartbeat, usually with a heart rate above 100 beats per minute for adults. Tachycardia accompanied by disturbance in the cardiac depolarization (cardiac arrhythmia) is called tachyarrhythmia.Sepsis in Children, and abdominal rigidityAbdominal RigidityAcute Abdomen. LipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion and amylaseAmylaseA group of amylolytic enzymes that cleave starch, glycogen, and related alpha-1, 4-glucans.Digestion and Absorption may be elevated, but not to the degree seen in acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis. Diagnosis relies on imaging, which will show extraluminal gas. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship require antibiotics and emergency surgery for repair.
Acute mesenteric ischemiaAcute Mesenteric IschemiaMesenteric Ischemia: tissue injury caused when perfusion fails to meet the demands of the intestines, usually due to an embolism or thrombosisThrombosisFormation and development of a thrombus or blood clot in the blood vessel.Epidemic Typhus. PatientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship have periumbilical painPainAn unpleasant sensation induced by noxious stimuli which are detected by nerve endings of nociceptive neurons.Pain: Types and Pathways out of proportion to the exam. Computed tomography with angiographyAngiographyRadiography of blood vessels after injection of a contrast medium.Cardiac Surgery is used to detect vessel stenosisStenosisHypoplastic Left Heart Syndrome (HLHS) or occlusion. LipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion can be elevated, but not to the degree seen in acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis. Acute ischemiaIschemiaA hypoperfusion of the blood through an organ or tissue caused by a pathologic constriction or obstruction of its blood vessels, or an absence of blood circulation.Ischemic Cell Damage requires revascularizationRevascularizationThromboangiitis Obliterans (Buerger Disease) and resection of the infarcted bowel.
Pancreatic cancer: a neoplasm of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy. Symptom onset is more insidious, and patientsPatientsIndividuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures.Clinician–Patient Relationship may have unrelenting epigastric painEpigastric painMallory-Weiss Syndrome (Mallory-Weiss Tear), weight lossWeight lossDecrease in existing body weight.Bariatric Surgery, and jaundiceJaundiceJaundice is the abnormal yellowing of the skin and/or sclera caused by the accumulation of bilirubin. Hyperbilirubinemia is caused by either an increase in bilirubin production or a decrease in the hepatic uptake, conjugation, or excretion of bilirubin. Jaundice. The diagnosis is confirmed with imaging. The history, exam, and imaging will differentiate pancreatic cancer from acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis. Treatment is usually aggressive because tumors are usually found late, and includes chemotherapyChemotherapyOsteosarcoma, radiationRadiationEmission or propagation of acoustic waves (sound), electromagnetic energy waves (such as light; radio waves; gamma rays; or x-rays), or a stream of subatomic particles (such as electrons; neutrons; protons; or alpha particles).Osteosarcoma, and surgery. PrognosisPrognosisA prediction of the probable outcome of a disease based on a individual’s condition and the usual course of the disease as seen in similar situations.Non-Hodgkin Lymphomas for survival is generally poor.
Billing and Coding
Diagnosis Codes:
These codes are used to diagnose acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, an acute inflammationAcute InflammationInflammation of the pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy. The codes can specify the cause, such as gallstonesGallstonesCholelithiasis (gallstones) is the presence of stones in the gallbladder. Most gallstones are cholesterol stones, while the rest are composed of bilirubin (pigment stones) and other mixed components. Patients are commonly asymptomatic but may present with biliary colic (intermittent pain in the right upper quadrant).Cholelithiasis or alcohol, and the severity.
Coding System
Code
Description
ICD-10-CM
K85.90
Acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis without necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage or infection, unspecified
ICD-10-CM
K85.10
Biliary acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis without necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage or infection
ICD-10-CM
K85.20
Alcohol induced acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis without necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage or infection
Evaluation & Workup:
These codes are for the key diagnostic laboratory tests. A markedly elevated serum lipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion is the most specific blood test for acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Coding System
Code
Description
CPT
83690
LipaseLipaseAn enzyme of the hydrolase class that catalyzes the reaction of triacylglycerol and water to yield diacylglycerol and a fatty acid anion. It is produced by glands on the tongue and by the pancreas and initiates the digestion of dietary fats.Malabsorption and Maldigestion
CPT
74177
Computed tomography, abdomen and pelvisPelvisThe pelvis consists of the bony pelvic girdle, the muscular and ligamentous pelvic floor, and the pelvic cavity, which contains viscera, vessels, and multiple nerves and muscles. The pelvic girdle, composed of 2 “hip” bones and the sacrum, is a ring-like bony structure of the axial skeleton that links the vertebral column with the lower extremities.Pelvis: Anatomy; with contrast material(s)
Complications:
These codes document the major local complications of severe acute pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis, such as the development of a pancreatic pseudocystPancreatic pseudocystCyst-like space not lined by epithelium and contained within the pancreas. Pancreatic pseudocysts account for most of the cystic collections in the pancreas and are often associated with chronic pancreatitis.Acute Cholangitis or necrotizing pancreatitisPancreatitisInflammation of the pancreas. Pancreatitis is classified as acute unless there are computed tomographic or endoscopic retrograde cholangiopancreatographic findings of chronic pancreatitis. The two most common forms of acute pancreatitis are alcoholic pancreatitis and gallstone pancreatitis.Acute Pancreatitis.
Coding System
Code
Description
ICD-10-CM
K86.3
Pseudocyst of pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy
ICD-10-CM
K85.31
Infected necrosisNecrosisThe death of cells in an organ or tissue due to disease, injury or failure of the blood supply.Ischemic Cell Damage of pancreasPancreasThe pancreas lies mostly posterior to the stomach and extends across the posterior abdominal wall from the duodenum on the right to the spleen on the left. This organ has both exocrine and endocrine tissue. Pancreas: Anatomy, early phase
Bollen, T. L., Singh, V. K., Maurer, R., Repas, K., van Es, H. W., Banks, P. A., Mortele, K. J. (2011). Comparative evaluation of the modified CT severity index and CT severity index in assessing severity of acute pancreatitis. AJR. American Journal of Roentgenology 197(2):386–392. https://doi.org/10.2214/AJR.09.4025
Crockett, S.D., Wani, S., Gardner, T.B., Falck-Ytter, Y., Barkun, A.N. (2018). American Gastroenterological Association Institute guideline on initial management of acute pancreatitis. Gastroenterology 154(4):1096–1101. doi: 10.1053/j.gastro.2018.01.032. Epub 2018 Feb 3. PMID: 29409760. https://www.gastrojournal.org/article/S0016-5085(18)30076-3/fulltext
Mortele, K.J., Wiesner, W., Intriere, L., et al. (2004). A modified CT severity index for evaluating acute pancreatitis: Improved correlation with patient outcome. AJR American Journal of Roentgenology 183:1261–1265. https://www.ajronline.org/doi/pdf/10.2214/ajr.183.5.1831261
Zhao, K., Adam, S., Keswani, R., Horowitz, J., Miller, F. (2015). Acute pancreatitis: revised Atlanta Classification and the role of cross-sectional imaging. AJR American Journal of Roentgenology 205(1):W32–W41. doi: 10.2214/AJR.14.14056. PMID: 26102416. https://www.ajronline.org/doi/pdf/10.2214/AJR.14.14056