Acute bronchiolitis is primarily a pediatric respiratory condition caused by inflammation of the bronchioles in response to a viral infection. The condition is a common cause of hospitalization in children in the United States, with the majority of cases caused by respiratory syncytial virus (RSV). Patients usually present with upper respiratory symptoms, such as cough and congestion, and later develop lower respiratory signs, including dyspnea, wheezing, crackles, and hypoxia, for up to 10 days. Diagnosis is clinical and treatment is directed at improving oxygenation and hydration. As the disease course is self-limiting, acute bronchiolitis has good prognosis with appropriate management.
Last updated: May 26, 2025
Acute bronchiolitis Bronchiolitis Inflammation of the bronchioles. Pediatric Chest Abnormalities is a clinical constellation of respiratory symptoms (increased work of breathing Work of breathing Respiratory muscle contraction during inhalation. The work is accomplished in three phases: lung compliance work, that required to expand the lungs against its elastic forces; tissue resistance work, that required to overcome the viscosity of the lung and chest wall structures; and airway resistance work, that required to overcome airway resistance during the movement of air into the lungs. Work of breathing does not refer to expiration, which is entirely a passive process caused by elastic recoil of the lung and chest cage. Pulmonary Examination, wheezing Wheezing Wheezing is an abnormal breath sound characterized by a whistling noise that can be relatively high-pitched and shrill (more common) or coarse. Wheezing is produced by the movement of air through narrowed or compressed small (intrathoracic) airways. Wheezing, and crackles) caused by acute inflammation Acute Inflammation Inflammation of the small airways (small bronchi Bronchi The larger air passages of the lungs arising from the terminal bifurcation of the trachea. They include the largest two primary bronchi which branch out into secondary bronchi, and tertiary bronchi which extend into bronchioles and pulmonary alveoli. Bronchial Tree: Anatomy and bronchioles Bronchioles The small airways branching off the tertiary bronchi. Terminal bronchioles lead into several orders of respiratory bronchioles which in turn lead into alveolar ducts and then into pulmonary alveoli. Bronchial Tree: Anatomy), typically secondary to viral infections Infections Invasion of the host organism by microorganisms or their toxins or by parasites that can cause pathological conditions or diseases. Chronic Granulomatous Disease.
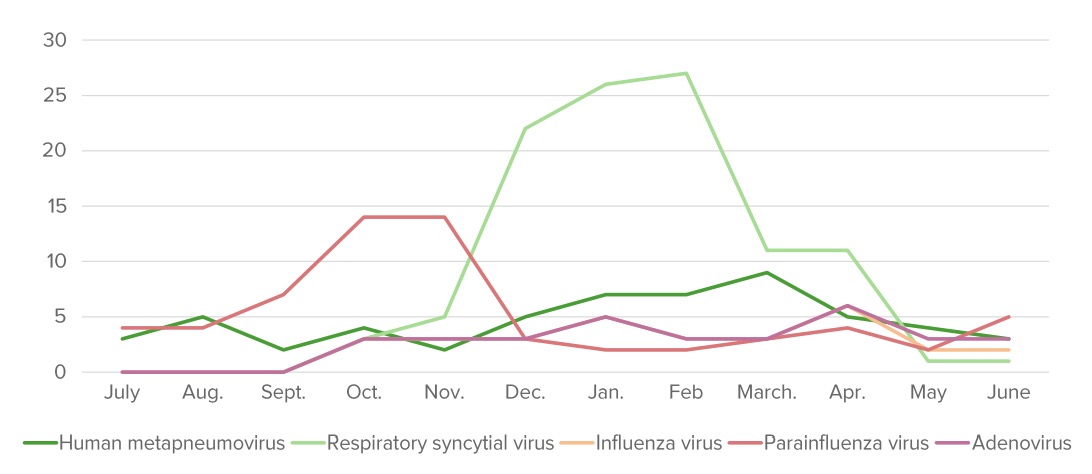
The annual distribution (%) of pathogens that cause bronchiolitis. “Bronchiolitis season” starts around October and finishes around May in the Northern Hemisphere.
Image by Lecturio.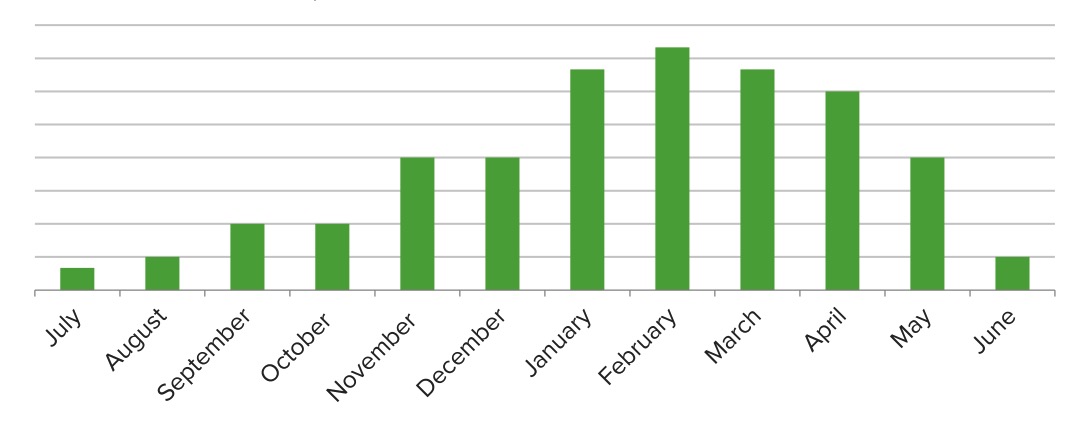
Seasonal variations in the number of cases that can be attributed to the respiratory syncytial virus (RSV): At its peak, RSV accounts for about 1/3 of bronchiolitis cases.
Image by Lecturio.Pathologic changes are noted within 24 hours of contact with a pathogen:
Symptoms are on a spectrum based on the severity of the disease:
Risk stratification at admission is important to determine the appropriate level of care.
Management depends on severity:
Diagnosis Codes:
These codes are used to document a diagnosis of acute bronchiolitis Bronchiolitis Inflammation of the bronchioles. Pediatric Chest Abnormalities, a common viral lower respiratory tract infection in infants and young children, most frequently caused by Respiratory Syncytial Virus Respiratory Syncytial Virus Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus ( RSV RSV Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus).
| Domain | Code | Description |
|---|---|---|
| ICD-10-CM | J21.0 | Acute bronchiolitis Bronchiolitis Inflammation of the bronchioles. Pediatric Chest Abnormalities due to respiratory syncytial virus Respiratory Syncytial Virus Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus ( RSV RSV Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus) |
| ICD-10-CM | J21.9 | Acute bronchiolitis Bronchiolitis Inflammation of the bronchioles. Pediatric Chest Abnormalities, unspecified |
| SNOMED CT | 26647002 | Acute bronchiolitis Bronchiolitis Inflammation of the bronchioles. Pediatric Chest Abnormalities (disorder) |
Evaluation & Workup:
This CPT code is for a rapid antigen Antigen Substances that are recognized by the immune system and induce an immune reaction. Vaccination test for RSV RSV Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus, performed on a nasal swab. While the diagnosis of bronchiolitis Bronchiolitis Inflammation of the bronchioles. Pediatric Chest Abnormalities is primarily clinical, identifying RSV RSV Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus can be useful for cohorting patients Patients Individuals participating in the health care system for the purpose of receiving therapeutic, diagnostic, or preventive procedures. Clinician–Patient Relationship in a hospital setting.
| Domain | Code | Description |
|---|---|---|
| CPT | 87807 | Infectious agent antigen detection Antigen detection Respiratory Syncytial Virus by immunofluorescent assay; respiratory syncytial virus Respiratory Syncytial Virus Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus |
Medications:
This code is used to bill for palivizumab Palivizumab A humanized monoclonal antibody and antiviral agent that is used to prevent respiratory syncytial virus infections in high risk pediatric patients. Respiratory Syncytial Virus, a monoclonal antibody given as a monthly injection to prevent severe RSV RSV Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus disease in high-risk infants (e.g., premature infants Premature infants A human infant born before 37 weeks of gestation. Sudden Infant Death Syndrome (SIDS), those with congenital heart disease). It is for prevention, not treatment.
| Domain | Code | Description |
|---|---|---|
| CPT | 90378 | Respiratory syncytial virus Respiratory Syncytial Virus Respiratory syncytial virus (RSV) is an enveloped, single-stranded, linear, negative-sense RNA virus of the family Paramyxoviridae and the genus Orthopneumovirus. Two subtypes (A and B) are present in outbreaks, but type A causes more severe disease. Respiratory syncytial virus causes infections of the lungs and respiratory tract. Respiratory Syncytial Virus, monoclonal antibody, seasonal dose |
Complications & Supportive Procedures:
These codes are used to document the primary reasons for hospitalization Hospitalization The confinement of a patient in a hospital. Delirium in severe bronchiolitis Bronchiolitis Inflammation of the bronchioles. Pediatric Chest Abnormalities, including apnea (pauses in breathing), especially in young infants, and acute respiratory failure Respiratory failure Respiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure requiring oxygen support.
| Domain | Code | Description |
|---|---|---|
| ICD-10-CM | J96.00 | Acute respiratory failure Respiratory failure Respiratory failure is a syndrome that develops when the respiratory system is unable to maintain oxygenation and/or ventilation. Respiratory failure may be acute or chronic and is classified as hypoxemic, hypercapnic, or a combination of the two. Respiratory Failure, unspecified whether with hypoxia Hypoxia Sub-optimal oxygen levels in the ambient air of living organisms. Ischemic Cell Damage or hypercapnia Hypercapnia A clinical manifestation of abnormal increase in the amount of carbon dioxide in arterial blood. Neonatal Respiratory Distress Syndrome |
| ICD-10-CM | R06.81 | Apnea, not elsewhere classified |